Home » Articles posted by Wendy Jones (Page 9)
Author Archives: Wendy Jones
Timing of breastfeeds if taking medication
I keep getting emails/ Facebook messages that mothers have been advised to pump and dump their breastmilk for a period of time after taking medication in order to minimise / prevent exposure of the baby to the drug. This has often been undertaken when the drug is compatible with breastfeeding and resulted in the unnecessary exposure of the baby to formula milk.
For most drugs taken for more than 3 days the amount in milk is constant across 24 hours. So timing feeds with respect to breastfeeding or dumping of the breastmilk is pointless. The half life of a drug is very important but just one of the factors in determining the compatibility with normal breastfeeding. If you want to know more please consider buying “Breastfeeding and Medication”
pdf of information Timing of medication and breastfeeds
Timing of drugs with respect to medication does not help to minimise levels to which babies are exposed in chronic conditions. Although the time to maximum level is often quoted, drugs reach a steady state 3-5 days after therapy begins and the levels then remain constant across the 24-hour period. Just as it takes approximately 5 half- lives for a drug to leave the body totally, it takes 5 half-lives to reach steady state. Before this time the levels increase gradually with every dose until they reach this point. Trying to time feeds disrupts normal breastfeeding and may result in engorgement with no benefit in milk levels to which the baby will be exposed. See Fig 1 below
Fig 1 accumulation of drug until it reaches steady state after 5 half lives (here taken to be 24 hours)
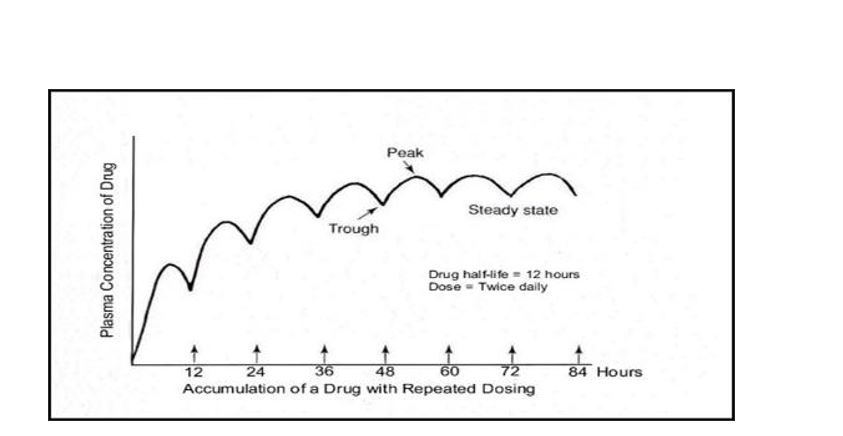
The half-life of a drug defines how long it takes to reach steady state and also how long it takes for it to be totally cleared from the mother’s body and milk. Five half-lives are taken as the closest measure in both cases.
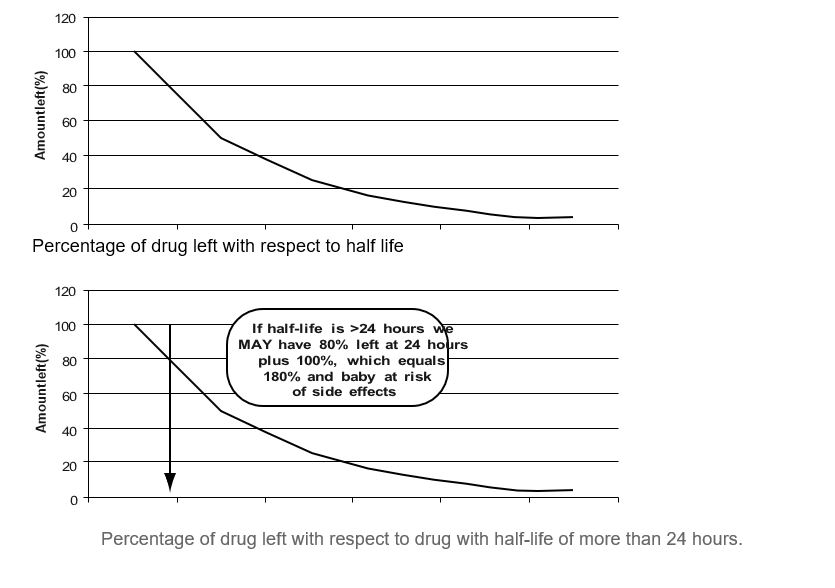
Fig 2 Percentage of drug left where half-life is 24 hours
If the half-life of the drug is more than 24 hours the level may begin to accumulate in the baby’s body and be more likely to produce adverse effects e.g. diazepam half-life 43 hours. Drugs with short half lives are preferred during breastfeeding. In general long acting / slow release formulations are better avoided if possible.
Fig 2 Percentage of drug left where half-life is 24 hours

Quetiapine and breastfeeding
One of the questions that comes up frequently. Often mothers told that they cannot breastfeeding if they need quetiapine for their own menatl health
Hope this information helps them make an infomed decision
PDF of factsheet available here
https://breastfeeding-and-medication.co.uk/wp-content/uploads/2022/06/quetiapine.pdf
The information on this sheet is based upon my professional experience as a pharmacist with a specialised interest in the safety of drugs in breastmilk, supported by evidence from expert sources. However, I cannot take responsibility for the prescription of medication which remains with the healthcare professionals involved. I am happy to discuss the evidence by email wendy@breastfeeding-and-medication.co.uk
Quetiapine is probably compatible with use during breastfeeding in dose less than 400mg daily based on limited studies and low theoretical infant dose. Be aware of possibility of drowsiness in the baby. Mother should not fall asleep with the baby in bed, on a settee or chair.
Bipolar disease description
Bipolar disorder is a mental health condition that affects moods. The latter can swing from one extreme of lethargy and depression to a feeling of being high and overactive hence the original name of manic depression. During bouts of depression, it is not uncommon to feel suicidal or worthless and it is important to recognise this and seek a place of safety or a person you trust as quickly as possible. During a manic phase there may be feelings of having lots of energy, ambitious plans and idea. It is not uncommon to spend large amounts of money on expensive, unwanted goods and some people ask their banks to block spending above a certain level to avoid debt. It is also common to not feel like eating or sleeping, to talk quickly and become easily annoyed. For some this phase is a positive experience and a time of creativity so may reject medication. It may also become a psychotic phase where things which do not exist may be seen and heard (voices controlling actions). It is a complex condition which may need adjustments. Around one in every 100 people will be diagnosed with it at some point in their life. It frequently develops between 15 and 19 years of age but rarely after 40. The incidence is the same in men and women. The pattern of mood swings in bipolar disorder varies widely. Some people only have a couple of episodes in their lifetime and are stable in between, while others have many episodes. Diagnosis is made only after one episode of mania as well as the depression. In this state the mother may have an elated mood or alternatively she may feel irritable and angry. She may experience racing thoughts rapidly changing from one area to another. It may be impossible for her to be still, but the activity may be unproductive. It is reported to affect a higher proportion of intelligent people with gifted creativity.
Quetiapine (Seroquel™)
Quetiapine is an Atypical anti-psychotic. Quetiapine may also be used in severe depression. In general, atypicals may be better tolerated with fewer extra-pyramidal side effects than the older drugs e.g., chlorpromazine and haloperidol . However, they do produce weight gain and a risk of hyperglycaemia which may need to be monitored regularly. Quetiapine has been associated with a low incidence of extra-pyramidal symptoms, but tardive dyskinesia may occur after long-term treatment. The most frequent adverse effects with quetiapine are somnolence and dizziness. Weight gain, particularly during early treatment, has also been noted. It appears to have a minimal effect on prolactin levels Lee et al. (2004) studied one mother taking 200 mg daily throughout pregnancy. Breastfeeding was not initiated in the absence of safety data until measurement of her breastmilk samples were available. Levels measured indicated that an exclusively breastfed baby would normally ingest only 0.09% of the weight adjusted dose (maximum 0.43%). The mother initiated breastfeeding 8 weeks after delivery. Follow up at 4.5 months indicated normal development with no adverse effects. Misri et al. (2006) studied six mothers taking 25 to 400 mg daily together with an antidepressant. In mothers taking less than 75 mg, milk levels were below the level of detection. One mother taking 400 mg daily had a level of drug in her milk of 101 µg per litre. Mental and psychomotor tests were below the norm in two of the infants when monitored up to 18 months of age although within the norm. The authors concluded this result was due to effects other than exposure to the drug. Several other case study reports of quetiapine use have been reported with low levels of drug reported in the babies and no adverse reactions directly attributable to the drug identified (Rampono et al. 2007; Kruninger et al. 2007; Balke 2001; Seppala 2004; Ritz 2005; Gentile 2006). A relative infant dose quoted as 0.070.1% is quoted (Hale online access).
Summary of Use during Lactation (LactMed https://www.ncbi.nlm.nih.gov/books/NBK501087/
Maternal quetiapine doses of up to 400 mg daily produce doses in milk that are less than 1% of the maternal weight-adjusted dosage. Limited long-term follow-up of infants exposed to quetiapine indicates that infants generally developed normally. A safety scoring system finds quetiapine to be possible to use during breastfeeding.[1] Systematic reviews of second-generation antipsychotics concluded that quetiapine seemed to be the first- or second-choice agent during breastfeeding.[2-4] Monitor the infant for drowsiness and developmental milestones, especially if other antipsychotics are used concurrently. E Elactancia https://www.e-lactancia.org/breastfeeding/quetiapine-fumarate/product/ Quetiapine is excreted into breast milk in clinically insignificant amounts. (Yazdani 2018, Aydin 2015, Van Boekholt 2015, Rampono 2007, Misri 2006, Lee 2004, Seppala 2004). Clinical or development problems in infants whose mothers were treated have not been observed, whether at the short or long term. (Levesque 2016, Sharma 2016, Aydin 2015, Van Boekholt 2015, Newport 2009, Rampono 2007, Misri 2006, Ritz 2005, Gentile 2005, Seppala 2004, Lee 2004). Very low plasma-levels of quetiapine in these infants were found. (Rampono 2007). Galactorrhoea may occur with or without an increase of prolactin. (Glocker 2021, Suttajit 2013, Mushtaq 2012, Sethi 2010, Gupta 2007, Atmaca 2002). Expert authors consider the use of quetiapine to be safe or very probably safe during breastfeeding. (Hale, Lactmed, Uguz 2021, Teodorescu 2020, Rybakowski 2019, Pacchiarotti 2016, Schaefer 2015, Grover 2005, Larsen 2015, Parikh 2014, Rowe 2013) Pharmacokinetics (Hale) Quetiapine is 83% plasma protein bound. The half-life is 6 to 7 hours. Milk plasma ratio 0.3. Relative infant dose 0.02% – 0.1% Other a typical drug options • risperidone (Risperidal™): Limited information indicates that maternal risperidone doses of up to 6 mg daily produce low levels in milk. Observe baby for drowsiness but no adverse events reported to date. • olanzapine (Zyprexa™): Maternal doses of olanzapine up to 20 mg daily produce low levels in milk and undetectable levels in the serum of breastfed infants. Monitor the baby for drowsiness and effective feeding. • aripiprazole (Ablify ™): Limited information indicates that maternal doses of aripiprazole up to 15 mg daily produce low levels in milk. However, it inhibits prolactin levels and despite expert advice it may not be possible to achieve a full milk supply ((Mendhekar 2006, Nordeng 2014). References
• Balke LD, Quetiapine effective in the treatment of bipolar affective disorder during pregnancy, World J Biol Psychiatry, 2001;2:303S. Abstract P02115.
• Drugs and Lactation Database (LactMed) https://www.ncbi.nlm.nih.gov/books/NBK501922/ • E Elactancia https://www.e-lactancia.org/
• Gentile S, Quetiapine-fluvoxamine combination during pregnancy and while breastfeeding, Arch Women’s Ment Health, 2006;9:158–9.
• Hale TW Medications and Mothers Milk online access Springer Publishing
• Jones W Breastfeeding and Medication Routledge 2018 • Jones W Breastfeeding and Chronic Medical Conditions Amazon 2020
• Kruninger U, Meltzer V, Hiemke C et al. [Pregnancy and lactation under treatment with quetiapine Psychiatr Prax Suppl, 2007;34:S756.
• LactMed
• Lee A, Giesbrecht E, Dunn E, Ito S, Excretion of quetiapine in breastmilk, Am J Psychiatry, 2004;161:17156.
• Misri S, Corral M, Wardrop AA, Kendrick K. Quetiapine augmentation in lactation: a series of case reports. J Clin Psychopharmacol. 2006;26:508-11.
• Pacchiarotti I, Leon-Caballero J, Murru A et al. Mood stabilizers and antipsychotics during breastfeeding: Focus on bipolar disorder. Eur Neuropsychopharmacol. 2016;26:1562-78
• Rampono J, Kristensen JH, Ilett KF, Hackett LP, Kohan R, Quetiapine and breastfeeding, Ann Pharmacother, 2007;41:7114.
• Ritz S, Quetiapine monotherapy in post-partum onset bipolar disorder with a mixed affective state, Eur Neuropsychopharmacol, 2005;15 (Suppl. 3):S407. Abstract.
• Seppala J, Quetiapine (‘Seroquel’) is effective and well tolerated in the treatment of psychotic depression during breastfeeding, Int J Neuropsychopharmacol, 2004;7 (Suppl. 1):S245. Abstract P01.431.
Specialist Pharmacy Service Safety in Lactation: Antipsychotics 2020
https://www.sps.nhs.uk/articles/safety-in-lactation-antipsychotics/
E Lactancia Quetiapine : https://www.e-lactancia.org/breastfeeding/quetiapine-fumarate/product/ : Very low risk
Asthma and Breastfeeding
As a community pharmacist I often saw patients repeatedly ordering their blue inhalers to relieve symptoms of asthma because they were scared that the brown preventer inhalers contained steroid and would make them look like body builders. This is, of course not going to happen using inhalers correctly. Oral thrush can be common if inhaler technique is poor but simple things like rinsing the mouth after use or using a spacer can help. Talk to your specialist asthma nurse if you are struggling with symptoms.
If we add in breastfeeding it is no surprise that mothers are concerned about their medication use to control asthma but without cause. Inhalers and steroids are compatible with breastfeeding. Not only that but breastfeeding helps to minimise the risk of your baby developing asthma in the future according to new research.
The symptoms of asthma being high because of very high pollen counts coupled with the risk of thunderstorms which can be a bad combination.
I hope this factsheet taken largely from Breastfeeding and Chronic Medical Conditions helps
wendy@breastfeeding-and-medication.co.uk
https://breastfeeding-and-medication.co.uk/wp-content/uploads/2022/06/asthma-.pdf
“My asthma actually improves when feeding and I had a big decline when I weaned my 2-year-old twins. The symptoms have gone again now I’m breastfeeding my 3-month-old.”
Description
Breastfeeding protects against asthma in children up to the age of 6. Shorter duration and non-exclusivity of breastfeeding were associated with increased risks of asthma-related symptoms in pre-school children (Mukherjee 2016). Thus, mothers with asthma may be keen to breastfeed exclusively to protect their baby. In a study of 366 pregnancies, symptoms worsened in 36% of women (Schatz 1988). Further studies by Schatz (1995) and Wendel (1996) in the United States suggest that 11–18% of pregnant women with asthma will have at least one emergency department visit for acute asthma and, of these, 62% will require hospitalisation.
Wilson et al (2022) studied 2021 mother-child dyads. Women reported the duration of any and exclusive breastfeeding and child asthma outcomes during follow-up at child aged 4 to 6 years. Outcomes included current wheeze (previous 12 months), ever asthma, current asthma (having ≥2 of current wheeze, ever asthma, medication use in past 12-24 months), and strict current asthma (ever asthma with either or both current wheeze and medication use in past 12-24 months). They showed that longer duration of exclusive breastfeeding had a protective association with child asthma.
Treatment
Asthma can be controlled during breastfeeding with:
- inhalers (short and long-acting beta 2 agonists to relieve symptoms
- bronchodilators to prevent symptoms
- compound inhalers,
- Prednisolone
- Leukotriene receptor antagonists.
Beta-adrenoreceptor agonists relieve symptoms of asthma attack such as breathlessness: E.g., Salbutamol, Bambuterol , Formoterol, Salmeterol, Terbutaline.The inhalers act locally in the lungs and limited transfer into blood let alone milk –
Oral Corticosteroids : Prednisolone – limited transfer at 40mg/day, higher doses short term. Very high doses or long term wait 4 hours after administration to breastfeed (but rarely necessary in my experience)
Inhaled Corticosteroid Inhalers prevent asthma symptoms and are used when regular use of preventer inhalers is necessary: E.g., Beclometasone, Budesonide, Fluticasone, Mometasone. Inhalers act locally in lungs and limited transfer into blood let alone milk
Leukotrine Receptor antagonists: Montelukast – relative infant dose 0.68%. Used in children so compatible with breastfeeding. However, in September 2019 the MHRA added a caution to use in children so individual mothers may need to decide for themselves if they wish to take this drug whilst breastfeeding.
“Healthcare professionals are advised to be alert for neuropsychiatric reactions, including speech impairment and obsessive-compulsive symptoms, in adults, adolescents, and children taking montelukast. The risks and benefits of continuing treatment should be evaluated if these reactions occur. Patients should be advised to read the list of neuropsychiatric reactions in the information leaflet and seek immediate medical attention if they occur.”
Zafirlukast– relative infant dose 0.7%. Absorption slowed with food. Used in children > 12 years so compatible with breastfeeding assumed.
Theophylline/ Aminophylline – prolonged half-life in neonates (babies < 6 weeks). One reported case of irritability. Avoid if possible, especially with young babies .
There are many options of inhalers and asthma specialist should be able to make symptoms changing life a rare rather than common event. Many athletes have asthma and are able to control symptoms with the right balance of medication. For some symptoms are worse with respiratory infections, for others season affects are greater e.g., moulds, pollen from different plant affecting different times of the year.
References
- Mukherjee M, Stoddart A, Gupta RP, Nwaru BI, Farr A, Heaven M, Fitzsimmons D, Bandyopadhyay A, Aftab C, Simpson CR, Lyons RA, Fischbacher C, Dibben C, Shields MD, Phillips CJ, Strachan DP, Davies GA, McKinstry B, Sheikh A, The epidemiology, healthcare and societal burden and costs of asthma in the UK and its member nations: analyses of standalone and linked national databases, BMC Medicine, 2016;14:113–128.
- Schatz M, Harden K, Forsythe A, Chilingar L, Hoffman C, Sperling W, Zeiger RS, The course of asthma during pregnancy, post-partum, and with successive pregnancies: a prospective analysis, J Allergy Clin Immunol, 1988;81:509–17.
- Schatz M, Zeiger RS, Hoffman CP, Harden K, Forsythe A, Chilingar L, Saunders B, Porreco R, Sperling W, Kagnoff M, Perinatal outcomes in the pregnancies of asthmatic women: a prospective controlled analysis, Am J Respir Crit Care Med, 1995;151:1170–4.
- Wendel PJ, Ramin SM, Barnett-Hamm C, Rowe TF, Cunningham FG, Asthma treatment in pregnancy: a randomized controlled study, Am J Obstet Gynecol, 1996;175:150–4.
- Wilson K, Gebretsadik T, Adgent MA, et al. The association between duration of breastfeeding and childhood asthma outcomes. Annals of Allergy, Asthma & Immunology. (https://www.annallergy.org/article/S1081-1206(22)00400-8/fulltext)
- https://www.sps.nhs.uk/articles/using-inhaled-or-topical-corticosteroids-during-breastfeeding/
Further information:
Asthma UK https://www.asthma.org.uk/
Norethisterone and breastfeeding
Many mothers take norethisterone to delay periods before holidays or even their wedding. Others use it to stop heavy bleeding and wish to continue to breastfeed.
Norethisterone and breastfeeding factsheet
Norethisterone 5mg tablets (Primolut N®, Utovlan®) is often prescribed to delay periods. This might be requested by the breastfeeding mother for example before a holiday or a wedding. There is little information from the research databases to support the use at this dose in breastfeeding. The only references are significantly lower doses (350mcg daily) used in progesterone only contraceptives.
It is suggested in the literature that this dose of norethisterone may reduce the quantity of breastmilk. In my experience a few mothers have noticed a temporary dip in supply but with holidays and weddings a change of routine could account for such a change. There seems to be no risk to the breastfeeding baby of a short course of medication at this dose.
Studies suggest that lower doses do not affect the composition of milk (reported in LACTMed. However Hale (Medications and Mother’s Milk states that although it is believed to be secreted into breast milk in small amounts, it may reduce lactose content and reduce overall milk volume and nitrogen/protein content, resulting in lower infant weight gain, although these effects are unlikely if doses are kept low. Norethisterone is a component of progestin oral contraceptives (Eg. Micronor™ and Brevinor ™ )
BNF : Postponement of menstruation 5mg norethisterone 3 times daily starting 3 days before expected onset (menstruation occurs 2–3 days after stopping)
N.B This information is based on anecdote and not research based studies
References
- https://www.e-lactancia.org/breastfeeding/norethisterone/product/
- https://www.ncbi.nlm.nih.gov/books/NBK501291/
- Jones W Why Mother’s Medication Matters
- Jones W Breastfeeding and Medication
Anti platelet drugs and breastfeeding
Although it is rare for a young woman to experience a heart attack, transient ischaemic attack or stroke, it does happen. They are usually prescribed anti-platelet drugs and until recently we found difficulty in providing information. However, this is the most up to date information which I have sourced and hope it helps anyone in this most difficult position.
pdf of factsheet Anti platelet drugs and breastfeeding factsheet
Anti-platelet drugs decrease platelet aggregation (stickiness) and may stop thrombus (clot)
formation. Clopidogrel is also used, sometimes alone or in combination with low-dose aspirin. There are unfortunately some mothers who, whilst breastfeeding, have a heart attack, transient ischaemic attack, stroke or other event that requires anti-platelet agents if only temporarily. Anti-platelets may also be given during investigation if such a condition is strongly suspected.
Aspirin dispersible 75 mg
Aspirin 75 mg acts by decreasing platelet stickiness irreversibly inhibiting aggregation. It is not used during treatment of thrombosis but may be used to after a myocardial infarction (MI), transient ischaemic attack and stroke or to decrease cardiovascular risk. It is also used to prevent recurrent miscarriage, with a past history of pre-eclampsia and other reasons in pregnancy (https://breastfeeding-and-medication.co.uk/fact-sheet/low-dose-aspirin-and-breastfeeding). Aspirin is not recommended during breastfeeding at analgesic doses of 600 mg four times a day, due to its association with Reye’s syndrome. However, use of low dose aspirin is considered acceptable. In the absence of the theoretical risk of association with Reye’s syndrome, aspirin would be a drug compatible with lactation due to its pharmacokinetic properties.
Milk Plasma ratio is 0.03-0.08, oral bio availability 50-75%, plasma protein binding 88-93%, relative infant dose 2.5% – 10.8%. There is no documented risk of association with Reye syndrome. Virtually all aspirin is metabolised 2-3 hours after dose.
Clopidogrel (Brand name: Plavix®)
Little is known about the levels of clopidogrel secreted into breastmilk but it’s likely to be a small amount (https://www.nhs.uk/medicines/clopidogrel/). Clopidogrel irreversibly modifies the platelet adenosine diphosphate (ADP) receptor. There are no human studies, but rat studies have shown passage into milk. This significance in human treatment is unknown. It’s unlikely that clopidogrel will cause any side effects in the baby. It is used with good tolerance in paediatrics, even in new-borns and infants (https://www.e-lactancia.org/breastfeeding/clopidogrel/product/)
The pharmacokinetics of clopidogrel show a low oral bio availability 50%, plasma protein binding 98%. Babies exposed to clopidogrel through their mother’s breastmilk should be monitored for rare bruising on the skin, blood in urine, vomit or stool.
Gastric irritation of aspirin and clopidogrel
Both aspirin and clopidogrel (Plavix ™) are gastro irritant so may need to be used with a proton pump inhibitor (PPI) for protection of the stomach. There has in the past been some concern over a potential interaction between clopidogrel and omeprazole and esomeprazole, with the anti-platelet effect of clopidogrel being diminished (https://www.gov.uk/drug-safety-update/clopidogrel-andproton-pump-inhibitors-interaction-updatedadvice#:~:text=Concomitant%20use%20of%20clopidogrel%20and,therapies%20would%20be%20mo
re%20suitable.) .
The Specialist Pharmacy Service suggest that this is a clinical decision but that
pantoprazole, lansoprazole and rabeprazole are suitable alternatives
(https://www.sps.nhs.uk/articles/do-proton-pump-inhibitors-reduce-the-clinical-efficacy-ofclopidogrel-2/). PPI medication is largely destroyed in the maternal gut and can be used during lactation.
Other anti-platelet drugs
- Prasugrel (Effient) No studies on the transfer of prasugrel into breastmilk are available
- Ticagrelor (Brilinta) No studies on the transfer of prasugrel into breastmilk are available
- Dipyridamole No studies on the transfer of prasugrel into breastmilk are available
References
- CKS Anti platelet treatment https://cks.nice.org.uk/topics/antiplatelettreatment/management/secondary-prevention-of-cvd/
- Elactancia https://www.e-lactancia.org/
- Finkelstein Y, Nurmohamed L, Avner M, Benson LN, Koren G. Clopidogrel use in children. J
Pediatr. 2005 https://pubmed.ncbi.nlm.nih.gov/16291359/ - Hale Medications and Mothers Milk Online Access
- Kwok CS, Loke YK, Effects of proton pump inhibitors on platelet function in patients receiving
clopidogrel: a systematic review, Drug Saf, 2012;35(2):127–39. - Kwok CS, Loke YK, Inconsistencies surrounding the risk of adverse outcomes with
concomitant use of clopidogrel and proton pump inhibitors, Expert Opin Drug Saf,
2012;11(2):275–84. - LactMed https://www.ncbi.nlm.nih.gov/books/NBK501922/
- LactMed Lansoprazole https://www.ncbi.nlm.nih.gov/books/NBK501283/
- LactMed Pantoprazole https://www.ncbi.nlm.nih.gov/books/NBK501280/
- LactMed Rabeprazole https://www.ncbi.nlm.nih.gov/books/NBK501282/
- Li JS, Yow E, Berezny KY, Bokesch PM, Takahashi M, Graham TP Jr, Sanders SP, Sidi D, Bonnet
D, Ewert P, Jennings LK, Michelson AD; PICOLO Investigators. Dosing of clopidogrel for
platelet inhibition in infants and young children: primary results of the Platelet Inhibition in - Children On clopidogrel (PICOLO) trial. Circulation. 2008
- https://pubmed.ncbi.nlm.nih.gov/18195173/
- NHS Clopidogrel. https://www.nhs.uk/medicines/clopidogrel/
- Patient Info Antiplatelet Drugs https://patient.info/doctor/antiplatelet-drugs

Domperidone as a galactogogue
Many women report lowered milk supply ( perceived or actual) and it is a cause of many contacts to breastfeeding experts and sadly a reason many mothers turn to formula when they hadnt intended. Domperidone has for a long time been recommended to help increase supply by utilsising its ability to increase prolactin. It shouldnt be used, in my opinion unless the mother has been supported to achieve regular and effective breastfeeding. It may be needed where a premature baby has been delivered and the mother has been pumping long term – many times the supply starts to dip after 2 weeks.
pdf of this information:
I wrote a factsheet for BfN looking at all the studies on study outcomes some years ago (https://www.breastfeedingnetwork.org.uk/domperidone/ ) . This information is an update on my thoughts and in light of experience and new reports.
Some years ago I wrote a factsheet for the Breastfeeding Network on the use of domperidone as a galactagogue when the recommendations for the use of domperidone changed
https://www.breastfeedingnetwork.org.uk/domperidone/. The MHRA and EHRA recommended that domperidone be prescribed only in limited situations and at a maximum dose of 10mg three times a day for 7 days and not for breastfeeding mothers https://www.gov.uk/drug-safetyupdate/domperidone-risks-of-cardiac-side-effects.
Domperidone has long been used as a galactagogue to increase milk supply. Most of the evidence from studies lies with use to increase lactation after premature delivery but can be used later where breastfeeding got off to a difficult start such as separation of mother and baby. The research studies on domperidone and use to increase milk supply can be found in the BFN link. In my experience it had been used when adequate breastfeeding support had not been given and when feeding was not effective or frequent enough to stimulate supply. This should always be the first intervention and should be happening at every professional contact with a breastfeeding mother.
When should domperidone not be used ?
Domperidone interacts with other medication and should not be used:
- before assessment by someone skilled in breastfeeding support alongside expressing both
breasts, at least 8-10 times in 24 hours including overnight - where either mother or baby has any evidence of cardiac abnormalities and specifically
arrhythmia - where either is receiving other medications known to prolong QT interval or potent CYP3A4
inhibitors e.g., quinolone antibiotics, ketoconazole, fluconazole, macrolide antibiotics, SSRI
antidepressants (risk low with most commonly used ( Funk 2013) tricyclic antidepressants,
salbutamol (https://ggcmedicines.org.uk/media/uploads/ps_extra/pse_21.pdf) - where severe hepatic impairment has been identified in mother or baby
- where either mother or baby has high or low levels of potassium, or low levels of magnesium (https://ggcmedicines.org.uk/media/uploads/ps_extra/pse_21.pdf)
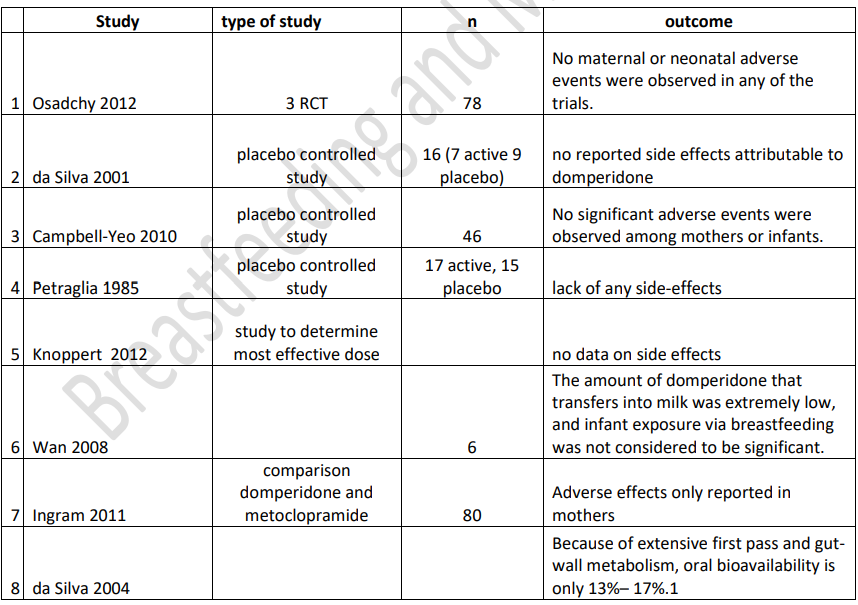
Are there adverse effects of domperidone on babies exposed through their mother’s milk? Hale data(2022) : milk plasma ratio 0.25% (<1 regarded as compatible with breastfeeding), plasma protein binding 93% leaving only 7% which can pass into milk, oral bioavailability 13-17% because of extensive first pass metabolism, relative infant dose 0.01%-0.35% (< 10% regarded as compatible with breastfeeding. Analysis of studies not complete but indicative of low risk to babies of domperidone passing to baby and would be grounds for use in breastfeeding to be reconsidered by EHRA and MHRA.
Higher doses of domperidone to increase milk supply?
Some breastfeeding experts have used significantly higher doses of domperidone to stimulate
lactation and continued use long term without reported adverse effects (Newman J, Polokova A What Doctors Don’t Know About Breastfeeding 2022)
Tapering off dose
There are no studies that provide an evidence base on how long to continue domperidone in the case of inadequate lactation (Academy of Breastfeeding Medicine (ABM) 2018 Anecdotally, some women feel that their supply cannot be maintained without the drug, while some can reduce the dose but not stop altogether. It is possible that domperidone is acting as a placebo to boost their confidence – we do not know and should admit the limitations of the research.
After a slow withdrawal from domperidone, one study found no significant increase in formula
supplementation suggesting that once sufficient milk production is established, it is maintained even without the use of domperidone (Livingston 2007).
Knoppert (2012) showed that in 3 out of 4 women who had taken domperidone for 4 weeks at full dose, 2 weeks at reducing dose, milk supply was maintained. Although gradual weaning from the drug has become standard, there is little published evidence apart from the reports and data is based on the experience of breastfeeding specialists.
Withdrawal
Drug withdrawal symptoms consisting of insomnia, anxiety, and tachycardia were reported in a woman taking 80 mg of domperidone daily for 8 months as a galactogogue who abruptly tapered the dose over 3 days (Papastergiou 2013).
Another mother (Seeman2015) took domperidone 10 mg three times daily for 10 months as a galactagogue and stopped abruptly. After discontinuation, she experienced severe insomnia, severe anxiety, severe cognitive problems and depression.
A third postpartum woman (Doyle 2018) began domperidone 90 mg daily, increasing to 160 mg daily to increase her milk supply. Because her milk supply did not improve, she stopped nursing at 14 weeks and began to taper the domperidone dosage by 10 mg every 3 to 4 days. Seven days after discontinuing domperidone, she began experiencing insomnia, rigors, severe psychomotor agitation, and panic attacks. She restarted the drug at 90 mg daily and tapered the dose by 10 mg daily each week. At a dose of 20 mg daily, the same symptoms recurred. She required sertraline, clonazepam and reinstitution of domperidone at 40 mg daily, slowly tapering the dose over 8 weeks. Three months were required to fully resolve her symptoms.
In a fourth case (Manzouri 2017), a mother took domperidone 20 mg four times daily for 9 months to stimulate breastmilk production. She stopped breastfeeding and domperidone at that time. Two weeks later, she presented with insomnia, anxiety, nausea, headaches and palpitations. The drug was restarted at a dosage of 20 mg three times daily and began to taper the daily dosage by 10 mg every week, but after one week she complained of insomnia. Tapering was reduced to 5 mg every week, but whenever she stopped the ndrug, symptoms returned. She was able to discontinue domperidone after tapering the daily dosage by 2.5 mg weekly over 10 months A fifth case (Sharma 2022) of a mother with a history of bipolar disorder and major depression developed severe anxiety, a recurrence of depression and obsessive compulsive disorder 6 days after abruptly discontinuing domperidone 120 mg daily that she was aking as a galactogogue. Three days later, she restarted domperidone 120 mg daily and tapered her daily dose by 10 mg at weekly intervals. She took no other medications. Two weeks after discontinuing domperidone, she had signs of only mild mood disorder. Hale (2022) reports an increase in calls to InfantRisk reporting problems with withdrawal after high dose and long-term use.
This should in my opinion be discussed with the mother before prescription of the medication.
References
- Academy of Breastfeeding Medicine ABM Clinical Protocol #9: Use of Galactogogues in
Initiating or Augmenting Maternal Milk Production, Second Revision Bodribb W 2018.
Breastfeed Med. 2018 Jun;13(5):307-314 - Asztalos EV, Kiss A, daSilva OP, Campbell-Yeo M, Ito S, Knoppert D; EMPOWER Study
Collaborative Group. Evaluating the Effect of a 14-Day Course of Domperidone on Breast
Milk Production: A Per-Protocol Analysis from the EMPOWER Trial. Breastfeed Med. 2019
Mar;14(2):102-107. doi: 10.1089/bfm.2018.0175. Epub 2018 Dec 13. PMID: 30543461. - Campbell-Yeo ML, Allen AC, Joseph KS et al. (2010) Effect of domperidone on the
composition of preterm human breast milk. Pediatrics 125(1): e107-114. - da Silva OP, Knoppert DC, Angelini MM et al. (2001) Effect of domperidone on milk production in mothers of premature newborns: a randomized, double-blind, placebo-controlled
trial. CMAJ 164(1): 17-21 - da Silva OP, Knoppert DC. (2004) Domperidone for lactating women. CMAJ 171(7): 725
- Doyle M, Grossman M. Case report: domperidone use as a galactagogue resulting in
withdrawal symptoms upon discontinuation. Arch Womens Ment Health. 2018
Aug;21(4):461-463. doi: 10.1007/s00737-017-0796-8. Epub 2017 Oct 31. PMID: 29090362. - Funk KA, Bostwick JR. A comparison of the risk of QT prolongation among SSRIs. Ann
Pharmacother. 2013 Oct;47(10):1330-41) - Grzeskowiak LE, Smithers LG, Amir LH, Grivell RM. Domperidone for increasing breast milk
volume in mothers expressing breast milk for their preterm infants: a systematic review and
meta-analysis. BJOG. 2018 Oct;125(11):1371-1378. doi: 10.1111/1471-0528.15177. Epub
2018 Mar 27. PMID: 29469929. - Grzeskowiak LE, Wlodek ME, Geddes DT. What Evidence Do We Have for Pharmaceutical
Galactagogues in the Treatment of Lactation Insufficiency?-A Narrative Review. Nutrients.
2019 Apr 28;11(5):974. doi: 10.3390/nu11050974. PMID: 31035376; PMCID: PMC6567188. - Hale TW and Krutsch K Medications and Mothers Milk 2022 Springer Publications
- Ingram J, Taylor H, Churchill C, Pike A, Greenwood R, Metoclopramide or domperidone for
increasing maternal breast milk output: a randomised controlled trial Arch Dis Child Fetal
Neonatal Ed F2 of 5(2011). doi:10.1136/archdischild-2011-300601 - Knoppert DC, Page A, Warren J, Carr M, Angelini M, Killick D, DaSilva OP, The Effect of Two
Different Domperidone Doses on Maternal Milk Production published online 3 May 2012 J
Hum Lact - Livingston V, Blaga Stancheva L, Stringer J. The effect of withdrawing domperidone on
formula supplementation. Breastfeeding Med. 2007; 2:278, Abstract 3.
Arnica (homeopathic)
Homeopathic arnica has been recommended for many years to relieve bruising and promote healing after birth. There is little research but historical use suggests that ” homeopathic products and topical application are usually safe during breastfeeding” LactMed https://www.ncbi.nlm.nih.gov/books/NBK501828/
Homeopathic remedies (https://kellymom.com/bf/can-i-breastfeed/herbs/natural-treatments/)
“Although there is little – if any – professional literature in this field on the use of homeopathic medicine, my reading and research has led me to the conclusion that these remedies pose minimal – if any – risk to the nursing baby. Homeopathic remedies are reportedly very safe for nursing moms and babies because the remedies (by definition of homeopathy) contain only very dilute versions of the active substances.
Most experts believe that homeopathic remedies are unlikely to pose a problem for the nursing baby and mother.”
Adults and children:2 pillules every 2 hours for the first 6 doses, then 4 times daily for up to 5 days or until symptoms improve https://www.nelsonspharmacy.com/arnicare-arnica-30c-clikpak. Although Nelsons website states that you should “Consult your doctor or pharmacist before taking this product if you are pregnant or breast feeding”
Arnica cream should not be applied to broken skin.
Psoriasis and Breastfeeding
pdf of this information available
Every time I see a doctor whether it be for me or the kids, they point it out. They will not give me anything for it until I stop feeding. Even had a 10-minute discussion about T-gel which I have now used so much it does nothing for me. I am so conscious of it xx
I have psoriasis myself, during the latter stages of my pregnancy it almost cleared. But was back the same as before within 12 weeks. My worst affected areas are my legs with smaller patches across my torso. I have noticed a few patches across breasts. I presume as a result of mild trauma from little hands. My daughter is 18 months ok now and still nurses.
UVB therapy helped me the first time and it cleared for months now it just makes it more manageable. I have only suffered with psoriasis for about 5 years. Steroid creams do not suit so I tend to use just moisturiser. Summer is awful as I still live in trousers as not comfortable to wear dresses or skirts.
My dermatologist refused everything last year when I went for a check. My daughter was 4 months old and I was told to just stop nursing. Needless to say, I refused, I am just itchy and scaly all the time.
I have suffered with psoriasis for 18 years. I had a difficult start to breastfeeding, but by week 7 things were starting to improve. I could actually enjoy feeds, instead of wincing in pain. Until one day I was in excruciating pain again. My psoriasis, for the first time in my life, had started to appear on my nipples and areola. No amount of lanolin cream helped. Feeds were so painful. So many tears! A GP told me to stop breastfeeding, I said it was not an option. So instead prescribed me a mild steroid and to stop feeding for a week and to exclusively pump instead. I had only JUST got my baby latching properly, I did not want to introduce a bottle and ruin it all! Luckily, a friend recommended coconut oil and within 2 days the psoriasis was clearing up and becoming less painful. Within 2 weeks it was gone!
I seriously thought my breastfeeding journey was over because of my condition. So many tears, so much ‘Mom guilt’. We are 6.5 months in now and only have to apply the oil once a week! I have also started Cimzia injections, which are safe for breastfeeding mothers. 6 weeks in and it is starting to clear up over the rest of my body too.
Description
Psoriasis is an epidermal thickening and scaling, frequently associated with silvery scales. The extensor surfaces – elbows, knees and lower back and scalp are commonly affected. Pitting of the nails occurs in 50% of patients. It may also develop on the genitalia. It cannot be transmitted by contact, but many people are wary of exposing plaques for fear that they may be stigmatised.
Some 2% of the population are affected and it most commonly begins < 35 years (peaking between 20 and 30 years). It is equally common in males and females but more common in the white population. Normally skin cells are replaced every 3-4 weeks, however, in psoriasis this occurs every 3-7 days leading to build up and plaque areas. It is believed to be an auto-immune condition.
Psoriasis may be triggered by certain drugs e.g. hydroxychloroquine, NSAIDs, beta blockers and ACE inhibitors. It may also be affected by hormonal changes — high levels of disease activity may be seen during puberty, post-partum, and during the menopause. Psoriasis typically improves during pregnancy, but in 10–20% of pregnant women psoriasis can worsen. It may also be triggered by trauma including tattoo or piercings, smoking and alcohol use (CKS Psoriasis 2018).
Treatment
Emollients help dryness, scaling and cracking of skin: compatible with breastfeeding
Shampoos with less contact time than creams and ointments are generally compatible with breastfeeding e.g. T gel ™ Alphosyl ™, Nizoral™, Selsun™
Salicylic acid: Keratolytic useful if there is significant scaling: No information is available on the clinical use of salicylic acid on the skin during breastfeeding. However, it is unlikely to be appreciably absorbed and so appear in breastmilk. It is considered compatible with breastfeeding
Topical steroids; Eumovate™, Betnovate™, Dermovate ™Dovobet (with betamethasone) ™: compatible with breastfeeding when applied in normal amounts
Coal Tar preparations. One study showed levels in baby’s urine, but absorption appeared to be due to contact with the products on skin rather than through breastmilk which showed no traces of coal tar (Scheeper 2009).
Dithranol, not to be used on flexures or the face. No data on levels in breastmilk
Vitamin D analogues: calcipotriol (Dovonex™), tacalcitol, and calcitriol (Silkis™): poorly absorbed after topical application, so probably a low risk to the nursing infant and is generally considered acceptable. Dovobet™ should not be applied to the nipples but can be applied elsewhere ( https://www.e-lactancia.org/breastfeeding/dovobet/tradename/).
Topical calcineurin inhibitors –
tacrolimus: presents a low risk to the nursing infant because it is poorly absorbed after topical application Ensure that the baby’s skin does not come into direct contact with the areas of skin that have been treated.
pimecrolimus: used in infants, poorly absorbed after topical application and plasma concentrations after topical so low risk to the nursing infant. Ensure that the baby’s skin does not come into direct contact with the areas of skin that have been treated
Vitamin A analogue (Tazarotene): Topical tazarotene has not been studied during breastfeeding.
Photochemotherapy (UVA) involves psoralen no data in breastfeeding
References
Scheepers PT, van Houtum JL, Anzion RB et al. Uptake of pyrene in a breast-fed child of a mother treated with coal tar. Pediatr Dermatol. 2009; 26:184-7
Further information
The Psoriasis and Psoriatic Arthritis Alliance www.papaa.org
Travel Sickness and Breastfeeding
Copy of this information is available as a pdf
As the summer season and travels begin, my mind has turned to travel sickness and breastfeeding. I suffer badly personally!
I hope this helps you enjoy your travels rather than dread them
Causes of travel sickness
Travel sickness or motion sickness happens when the body, the inner ear, and the eyes send conflicting signals to the brain. This most often happens when you are in a car, boat, or airplane, but it may also happen on flight simulators or amusement park rides.
It is more common in children and in women. Sitting in the back of the car can also be a trigger for many people or a on a coach. I personally find the new trains which are faster much harder to deal with as they seem to sway much more.
It is difficult as a breastfeeding mother to deal with your own travel sickness as well as a baby or children. You may be able to drive rather than be a passenger. If not ,then there are medications which you can take which wont reduce your supply (because only being used short term) or affect your baby. Some temporary drowsiness is possible with any medicine which makes you drowsy.
Symptoms of travel sickness
Symptoms can come on very suddenly but rapidly escalate:
- Nausea and vomiting
- Pale skin
- Cold sweats
- Dizziness
- Headache
- Increased salivation
- Fatigue
- Difficulty concentrating
- Rapid breathing
These are symptoms not dissimilar to panic.
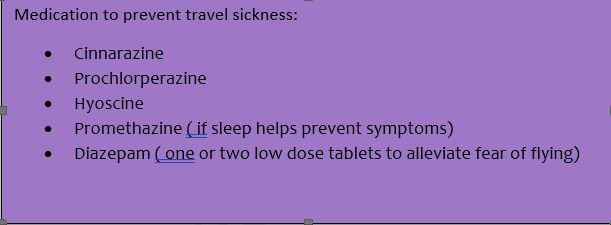
Medication
- If you are breastfeeding and need to care for a baby you may prefer one that is less likely to cause drowsiness – e.g. cinnarizine (Stugeron™)
- Hyoscine (Kwells ™, Joy Rides™) is usually regarded as the most effective medicine for motion sickness taken 30-60 minutes before the journey.
- Prochlorperazine (Buccastem™, Stemetil™)
- Cyclizine might be prescribed for you but is no longer available over the counter.
- Hyoscine patch can be prescribed. These are applied behind the ear 5-6 hours before travelling.
- Metoclopramide and domperidone may be useful to slow gastric emptying but are generally not prescribed for travel sickness.
- Homeopathic remedies e.g. Nelson’s Travella has limited research but is not harmful to the breastfed infant if it is a remedy which the mother finds useful.
- Antihistamines which cause drowsiness e.g. promethazine (Phenergan™, chlorpheniramine (Piriton ™) may be useful for children who struggle with travel sickness although it is rare before the age of 2 years.
Acupressure Bands
Some studies suggest that acupressure may help reduce symptoms of motion sickness in the same way as acupuncture. Acupressure bands are available commercially to help prevent motion sickness. Studies suggest these bands may help delay the onset of symptoms.
Traditionally, the acupuncture point known as Pericardium 6 is said to help relieve nausea. It is on the inside of the wrist, about the length of 2 fingernails up the arm from the centre of the wrist crease.
To reduce risk of travel sickness without medication
https://www.nhs.uk/conditions/motion-sickness/
- sit in the front of a car or in the middle of a boat.
- look straight ahead at a fixed point, such as the horizon rather than at a book, phone screen or portable device.
- fresh air e.g. open a car window
- close your eyes and breathe slowly while focusing on your breathing.
- distract children by talking, listening to music or singing songs.
- break up long journeys to get some fresh air, drink water or take a walk.
- some people recommend ginger, as a tablet, biscuit or tea but if you have had significant sickness in pregnancy this may bring back memories!
- Avoid heavy or fatty meals.
Fear of flying
One of the questions I have had frequently at this time of year has been about supporting the breastfeeding mother who has a fear of flying. I know this feeling myself so can empathise. I have always wanted to keep my headphones on and focus on breathing and listening to my music/relaxation most just when you are coming in to land and are told to take them off. I resort to counting backwards from a thousand.
However, diazepam as one or two low doses can be prescribed during breastfeeding. At worst the baby may temporarily be a little drowsy, but in practice this doesn’t seem to happen ( they are often too busy looking round and being social!)
Don’t forget to pack plastic bags or bowls ( just in case), wipes and cold water if the worst happens.
Entenox, safety for midwives and environmental impact
Having had the pleasure of presenting this on Matflix it has made me think a lot about the impact of entenox for midwives, for mothers and the environment.
You can access the matflix hour here
These are the slides I used