Home » Articles posted by Wendy Jones (Page 5)
Author Archives: Wendy Jones
Vomiting in pregnancy whilst still breastfeeding
PDF of this information is available at:
The Management of Nausea and Vomiting in Pregnancy and Hyperemesis Gravidarum (Green-top Guideline No. 69) Feb 2024
Thank you to everyone on the facebook group who shared their experiences and helped me to update this information.
More women are now breastfeeding their babies for longer and may still be feeding when they fall pregnant. For those who suffer from hyperemesis gravidarum (HG) this is a tough time. Sadly, some healthcare professionals do not understand that there is benefit to a child from being breastfed to the age of two years and beyond (WHO) alongside a normal weaning diet. Being asked to abruptly wean your older child in order to take medication is not an easy option and is not necessary. Sometimes sitting quietly to breastfeed whilst you fight the feeling of nausea is helpful. Some professionals remain concerned about the teratogenicity of drugs in pregnancy despite national guidance.
“ I had an absolutely awful time while still trying to breastfeed a toddler. The GP refused to prescribe anything other than cyclizine despite me calling them in desperation many times. Nothing else was made available and I was told that I just had to wait until it cleared up.”
Symptoms of NVP and HG
Nausea and vomiting of pregnancy (NVP) is common and usually settles by 12-14 weeks of pregnancy (although it may be longer and even last the full pregnancy). Often known as morning sickness it can occur at any time of the day or last all day.
Hyperemesis gravidarum is a severe form and can affect up to 1 to 3 in 100 pregnant women. Sadly, some women experience such extreme symptoms that they feel that they have no choice but to terminate the pregnancy even if it is a much longed for baby.
“I ended in termination of pregnancy after first hospital visit as I didn’t want to take from my child who was already here and after how badly I dealt with it last time, it being worse instantly I couldn’t do it”
Others decide that one child is sufficient to complete their family as they cannot contemplate symptoms again. There are medications but often primary care professionals do not appreciate the severity of symptoms or impact on mothers.
“I had HG with my daughter who will be 11 next month. Hyperemesis is the primary reason I only have one child. It was physically horrendous, and I had post-traumatic stress for years afterwards”.
“I had this with my daughter. It is the reason she will be an only child. She’s 4 now and I still suffer a lot of health issues as a direct result of hyperemesis. I had the best medical care. And was lucky to be given a lot of treatment. But it wasn’t enough, and my body still struggled. You can’t appreciate how difficult it is until you’ve experienced it.”
When asked in a facebook group (https://www.facebook.com/breastfeedingandmedication) for their experiences of suffering from morning sickness and hyperemesis, one of the overwhelming comments from women was about reluctance of GPs to prescribe medication in pregnancy, even when it had been prescribed whilst the mother was hospitalised!
“After one of my hospitalisations I was sent home with a prescription for cyclizine and when I went to my GP to renew the prescription she talked me out of it because “it wasn’t making enough of a difference for me to go back to work” so didn’t seem worth taking (mild relief from the symptoms of HG wasn’t considered a benefit.)”
Repeated comments from family, friends and professionals underestimated how the woman was feeling and she didn’t feel listened to.
“I didn’t feel I wasn’t listened to and also I didn’t feel dismissed. I just accepted this was part and parcel of my pregnancy as it was just relayed to me that it was normal.”
“It was awful. People (friends, family, healthcare workers) were quick to tell me what worked for them, and I felt very blamed that I was somehow not trying hard enough. All the admissions were almost a relief, just to lie there with fluid going in. I used to be admitted for several days each week, particularly in third trimester. I still have consequences from the prolonged malnutrition.”
For what should be a joyous family time there were repeated descriptions of an awful experience:
“ horrendous, hell on earth, pure hell, absolutely hell, housebound for months, nothing worked”.
“ I wasn’t taken seriously until my organs started to shut down and I needed to be induced, I spent 5 months in bed, couldn’t drink water or anything else, everything made me feel nauseous.”
“ I vomited so much and so hard that every time I wet myself and my nose bled. I was told when I was 5 weeks pregnant that if I didn’t want to be sick I shouldn’t be pregnant. I ended up hospitalized at 8 weeks.”
Should this be the experience of women in the UK in 2023?
Anti emetics in breastfeeding and pregnancy
Many of the drugs used to relieve nausea in pregnancy may be associated with lowering of milk supply. However, most women find that their supply very rapidly diminishes when they are pregnant. Many also develop aversion and very sensitive nipples and wish to limit feeding. Sadly, toddler nurslings don’t always understand the loss of their comfort! Many breastfeeding dyads continue to dry nurse throughout pregnancy and may go on to tandem feed. It is the decision which works for each family which matters, without judgement from family and professionals.
Hyperemesis may result in dehydration and subsequent admission to hospital. Signs of dehydration include feeling very thirsty, becoming drowsy or unwell, urine changing from a light yellow to a dark yellow or brown colour. Medical help should be sought if even sips of fluid produce vomiting. Weight loss can be excessive because of the restriction of quantity of food tolerated. Hyperemesis is diagnosed when there is prolonged nausea and vomiting with more than 5% pre pregnancy weight loss, dehydration and electrolyte imbalance. https://cks.nice.org.uk/topics/nausea-vomiting-in-pregnancy/background-information/definition/
Self-care
https://cks.nice.org.uk/topics/nausea-vomiting-in-pregnancy/management/management/
- Rest as needed and try to avoid sensory stimuli that may trigger symptoms, such as odours, heat, and noise.
- Try eating plain biscuits or crackers in the morning.
- Try eating bland, small, frequent protein-rich meals which are low in carbohydrate and fat.
- Cold meals may be more easily tolerated if nausea is smell-related.
- Drinking little and often, rather than large amounts.
- Ginger (can be taken in fresh, tea, capsule, or syrup form).
- Acupressure (such as over the P6 point on the ventral aspect of the wrist using a wrist band or finger pressure).
Responses on the facebook group as to how helpful these suggestions were are exemplified by:
“Nausea and sickness with my first born I had such a heightened sense of smell. I couldn’t even open my fridge without feeling sick and running to the loo. I ended up using a cool bag instead of my fridge, and I had to call my mum to come and help me when my partner was away. I couldn’t brush my teeth without gagging and wanting to be sick.”
“I was asked what is had to eat and when I said an oat/raisin bar the doctor replied I shouldn’t be having anything sugary. That one doctor who knew her stuff had told me to eat anything I could keep down.”
Medical Treatment
The RCOG green top guidelines on treating are available https://www.rcog.org.uk/media/y3fen1x1/gtg69-hyperemesis.pdf
The UKTIS information on the use of drugs in pregnancy can be found at https://www.medicinesinpregnancy.org/Medicine–pregnancy/NV/
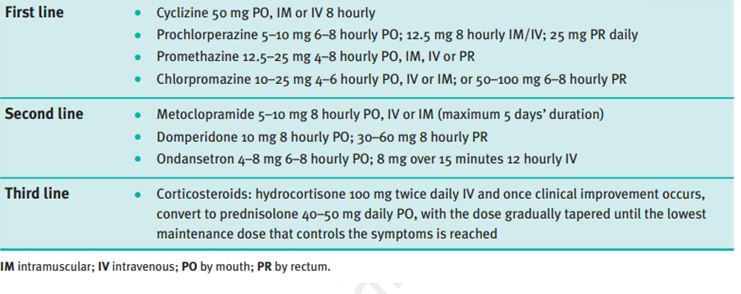
RCOG Recommended antiemetic therapies and dosages
In this fact sheet I have provided links to detailed information on the medication which can help prescribers to reach an evidence-based decision on the safety of the drug to the breastfeeding baby which is not available in standard reference texts like the British National Formulary (BNF). The linked pdf files contain information sourced from LACTMED February 2023
First Line treatments
- Cyclizine (Valoid™)
May possibly cause some drowsiness in the nursling but anecdotally appears to happen rarely . See https://www.ncbi.nlm.nih.gov/books/NBK501749/ and https://www.e-lactancia.org/breastfeeding/cyclizine/product/
Cyclizine is an anti-emetic used to treat nausea and vomiting including motion sickness, post-operative nausea and vomiting, after radiotherapy, in drug-induced situations, as well as for nausea in pregnancy. There are no reports of levels entering breastmilk (BNF) or data on which to base conclusions. There is an unlicenced dose for children aged over 6 years. It may be given orally, by IV or IM every 8 hours. Manufacturers advise to avoid in pregnancy, but there is no evidence of teratogenicity
·
Prochlorperazine (Buccastem, Stemetil)
Low levels of prochlorperazine are secreted into breastmilk and it can be used when breastfeeding. Side effects for the mother include drowsiness, restlessness and occasional extra pyramidal effects but babies seem to exhibit no adverse reactions. It is licensed to be given directly to babies weighing more than 10 kg. See https://www.ncbi.nlm.nih.gov/books/NBK501080/ and https://www.e-lactancia.org/breastfeeding/prochlorperazine/product/
Prochlorperazine is used to treat vertigo, labyrinthitis, migraine or drug-induced emesis if severe vomiting is a problem. Its oral bio-availability is low due to high first-pass metabolism but, like all phenothiazines, it has many metabolites, some active. It is not generally used in travel sickness prophylaxis. It is a member of the phenothiazine family to which children are particularly sensitive. Long-term use should be avoided in breastfeeding where possible, particularly with very young babies where there is a potential risk of apnoea. However, short-term acute use probably poses few risks as it is licenced for use in children over 10 kg. The dose is 5-10mg (one or two tablets) every 6-8 hours. It may also be given IV or IM.
- Promethazine (Avomine™ Phenergan™, Sominex™)
When used for hyperemesis in mother promethazine may possibly cause some drowsiness in the nursling but anecdotally appears to happen rarely. It also causes drowsiness in the mother so care should be taken with co sleeping.
See https://www.ncbi.nlm.nih.gov/books/NBK501081/ and https://www.e-lactancia.org/breastfeeding/promethazine/product/
Promethazine is widely used to reduce nausea particularly associated with travel sickness as well as symptomatic relief of urticaria and as an over-the-counter (OTC) hypnotic for short-term use. No data are available on transfer into breastmilk but it is believed that it does pass into breastmilk. It is licenced for use in children over 2 years.”
· Doxylamine/pyridoxine (Xonvea™)
This is the only licensed drug treatment for nausea and vomiting of pregnancy. It contains a combination of the antihistamine doxylamine and the vitamin pyridoxine. It became available in England in 2018. It has been widely used for pregnancy sickness in the US and Canada and studies have shown no link with birth defects in the baby. The antihistamine doxylamine might be more likely to cause drowsiness in nursling. https://www.ncbi.nlm.nih.gov/books/NBK500620/ and https://www.e-lactancia.org/breastfeeding/doxylamine-succinate/product/. The 10mg of pyridoxine is unlikely to cause any disruption to breastfeed.
Second Line Treatments
· Metoclopramide (Maxolon™)
Metoclopramide has also been used to increase milk supply. It is associated with an increased risk of depression as well as other side effects if used long term. There are no reports of problems in the babies from the amount passing through breastmilk. https://www.ncbi.nlm.nih.gov/books/NBK501352/
Metoclopramide is a dopamine antagonist and can cause extra-pyramidal side effects, in particular acute dystonia. This adverse effect is most commonly seen in children and young adults, especially females, so it is not a drug of choice in lactating mothers who generally fall into this age group. It may also precipitate hypotension and depression. Other side effects reported include headache, diarrhoea, dry mouth and change in appetite (Ingram et al. 2011). It stimulates prolactin secretion and has been used as a galactogogue but has now been superseded by domperidone because of the latter does not cross the blood–brain barrier (Ingram et al. 2012). The bio-availability of oral metoclopramide is about 75% but varies widely between patients due to its hepatic first-pass metabolism. Concentrations higher than those in maternal plasma may be reached in breastmilk, particularly in the early puerperium, although these decrease with increased maturity. Metoclopramide has pro-kinetic and anti-emetic properties and acts directly on the gastrointestinal tract without altering acid secretion. It is more frequently used in the US where domperidone is not available. Relative infant dose is quoted as 4.7–14.3% (Hale online access). The BNF states that only a small amount is present in breastmilk but it should be avoided.
· Domperidone (Motilium™)
Domperidone has widely been used to increase milk supply in the past. Concerns were raised by the MHRA in 2014 about use in patients with heart defects, there has been some reticence by doctors to prescribe it. There are no reports of problems in the amounts passing through breastmilk
See https://www.ncbi.nlm.nih.gov/books/NBK501371/ and https://www.e-lactancia.org/breastfeeding/domperidone/product/
Domperidone acts at the chemoreceptor trigger zone. It stimulates gastric emptying. It causes fewer central effects such as sedation and dystonia (although there are still reports of these) because it does not cross the blood–brain barrier as metoclopramide does. Its dopamine antagonist activity stimulates prolactin release, which makes it useful as a galactagogue (see section on drugs to increase lactation, pages 285–288). Domperidone is metabolised by cytochrome P450 so care should be taken with potential interactions. It is more than 90% bound to plasma proteins and has a low bioavailability on an empty stomach (15%) when taking orally due to first-pass hepatic and intestinal metabolism. Mean serum levels of domperidone measured in babies through maternal use of 10 mg three times daily was only 1.2 ng per millilitre. The total amount of the drug that would be ingested by the infant (Da Silva et al. 2001) would be extremely small (about 180 ng per kilogramme daily, assuming a daily milk intake of 150 ml per kilogramme). Relative infant dose quoted as 0.01– 0.04% (Hale 2017 online access). The BNF states that the amount secreted into breastmilk is probably too small to be harmful.
· Ondansetron (Zofran™)
This is an anti-emetic originally used to treat people who have severe sickness when being treated with chemotherapy for cancer. Ondansetron is frequently used for nausea during and after caesarean section, usually in doses of 4 to 8 mg intravenously. Use during and after caesarean section appears to not affect the onset of breastfeeding. No adverse infant effects have been reported or among women who received ondansetron postpartum in a pharmacokinetic study. Use of ondansetron in nursing mothers beyond the immediate postpartum setting has not been studied well, but the drug is licensed for use in infants as young as 1 month of age. See https://www.ncbi.nlm.nih.gov/books/NBK500798/ and https://www.e-lactancia.org/breastfeeding/ondansetron/product/
This drug is a 5-HT3 antagonist with antiemetic activity. It is also for the prevention and treatment of post-operative nausea and vomiting that have not responded to other antiemetic agents. Ondansetron may also be used for nausea in pregnancy. It is licenced for use in children It is 60% orally bio-available and 70–75% plasma protein bound. The terminal half-life is three hours after oral doses. There are no studies on transfer into breastmilk although it has been found in animal studies (BNF).
A large, well-designed study found that the vast majority of babies exposed to ondansetron in the womb (at least 998 out of every 1,000) are born without cleft lip and/or palate (https://www.medicinesinpregnancy.org/Medicine–pregnancy/Morning-Sickness/)
Third Line
Corticosteroids
Corticosteroids are sometimes prescribed for women with hyperemesis gravidarum that has not responded to other treatments including rehydration together with anti-emetics. There is no strong evidence that use of corticosteroids in early pregnancy increases the chance of cleft lip and palate or heart defects in the baby. Use in pregnancy also does not appear to increase the chance of the baby having a low birth weight. Some studies have shown that pregnant women taking corticosteroids have a higher chance of preterm delivery. However, it is thought that this is likely caused by the underlying illnesses that steroids are commonly used to treat rather than a direct effect of steroids themselves. https://www.medicinesinpregnancy.org/Medicine–pregnancy/Corticosteroids—systemic/
Pregnancy Sickness Support in the UK found that many women seeking terminations in desperation had not been offered the full range of treatments available and fewer than 10% had been offered steroids
Other non-medical treatments
· Ginger
The conclusion from 6 randomised controlled trials with a total of 675 participants was that ginger extract at 1000 mgs per day may be effective treatment for NVP. However , the small number of patients in these studies allocated to receive ginger (n=303) may have been insufficient to properly test the safety of ginger with regards to pregnancy outcome. ( Viljoen, E., Visser, J., Koen, N. et al. A systematic review and meta-analysis of the effect and safety of ginger in the treatment of pregnancy-associated nausea and vomiting. Nutr J 13, 20 (2014).) The authors found that Ginger did not significantly reduce the number of vomiting episodes during NVP, when compared to placebo, although there was a trend towards improvement. Many mothers have reported feeling angry and frustrated that this is recommended so frequently but that they found it caused side effects as well as not being effective. It is definitely not the answer to all NVP!
· Acupressure
Stimulation of the acupressure point, located three fingers breadth above the wrist, has been used for many years to treat nausea from a variety of causes. Mohd Nafiah et al (2022) concluded that the use of acupressure wristbands at the P6 point was also able to decrease the frequency of antiemetics and increase the rate of urine ketone clearance. The implication of the trial was the reported as the existence of an effective adjunct to alleviate the severity of nausea and vomiting in pregnant women with hyperemesis gravidarum, thereby improving their quality of life. There are no concerns about the safety of acupressure in pregnancy ( Mohd Nafiah, N.A.; Chieng, W.K.; Zainuddin, A.A.; Chew, K.T.; Kalok, A.; Abu, M.A.; Ng, B.K.; Mohamed Ismail, N.A.; Nur Azurah, A.G. Effect of Acupressure at P6 on Nausea and Vomiting in Women with Hyperemesis Gravidarum: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 10886.)
Conclusion
We should not underestimate how NVP and HG affect pregnant women. We should listen to how they are feeling and ask how we can help. Untreated symptoms can lead to lifetime mental health issues.
“I had morning sickness (not hyperemesis). The first 4 months I went from bed to the sofa, my husband did everything. I couldn’t look at food, walk into the kitchen to get a drink etc. I wasn’t physically that sick but the nausea was absolutely horrendous. Constantly, nothing stopping it, the minute I woke to the second I fell asleep for 4 months. I lost 6kg by my first scan. Although it got better I still felt slightly sick through the whole pregnancy. I was refused anti nausea meds by multiple doctors, even the midwife shrugged it off. The effect it has had on me even now (my daughter is 2.5) is horrible. I still can’t eat certain foods, put too much food in my mouth and the slightest nausea (which I get often due to anxiety, migraines etc) sends me into complete panic.”
“What would you like professionals to understand? The struggle and how debilitating it is.”
“Medically, only one doctor seemed to have any awareness of what I was suffering from. Others told me “I’d be better in a couple of weeks” every two weeks.”
Resources
Pregnancy Sickness Support https://www.pregnancysicknesssupport.org.uk/
RCOG Green Top Guidelines https://www.rcog.org.uk/guidance/browse-all-guidance/green-top-guidelines/the-management-of-nausea-and-vomiting-of-pregnancy-and-hyperemesis-gravidarum-green-top-guideline-no-69/
UKTIS Medicines in Pregnancy https://www.medicinesinpregnancy.org/About-Us/

Botox for medical purposes and Breastfeeding
Botox injections are used for many medical purposes including migraine, anal fissures. The amount of botox getting into milk is low based on the research on one mother who caught botulism from eating fermented salmon eggs. She continued to breastfeed. No botulinum toxin or botulism was found in the breastmilk or the baby. The doses that are used medically are far lower than that which would have caused the mother’s botulism so the amount in breastmilk is assumed to be too low to produce adverse effects.
Hale also comments that when Botox is injected into the muscle, it produces a partial chemical denervation resulting in paralysis of the muscle. When injected properly, and directly into the muscle, the toxin does not enter the systemic circulation. Thus levels in maternal plasma, and milk are very unlikely. Waiting a few hours for dissipation of any toxin would all but eliminate any risk to the infant. Also, avoid use of generic or unknown sources of botulinum toxin, as some are known to produce significant plasma levels in humans. (Hale TW Medications and Mothers Milk online version accessed Feb 2024)
In February 2024 a study of 4 mothers was published https://www.liebertpub.com/doi/abs/10.1089/fpsam.2023.0326
Objective: To detect the presence of botulinum toxin in breast milk from lactating subjects treated with facial botulinum toxin injections, as measured by enzyme-linked immunosorbent assay (ELISA).
Methods: For this pilot study, lactating women were injected with standardized facial botulinum toxin type A (BTXA) (range 40–92 U). Collected breast milk samples over 5 days were analyzed for the presence of botulinum toxin. Exclusion criteria included (1) lactating women still using their breast milk for their infant, (2) muscular disorders, (3) any medication that could interfere with neuromuscular function, (4) uncontrolled systemic disease, (5) pregnant, and (6) neuromodulator injection in the past 90 days.
Results: Four lactating women were recruited. Eight samples had no BTXA detected, whereas 8 of the 16 total had detectable amounts, which were well below the reported lethal oral dose for an infant.
Conclusion of the authors: Although the exclusion of lactating women from receiving cosmetic botulinum toxin injections is out of an abundance of caution to the theoretical risk to the infant, this study helps support the notion that facial botulinum toxin injections do not warrant an interruption in breastfeeding. Further studies with larger sample sizes are needed.
Hudson C, Wilson P, Lieberman D, Mittelman H, and Parikh S. Analysis of Breast Milk Samples in Lactating Women After Undergoing Botulinum Toxin Injections for Facial Rejuvenation: A Pilot Study.Facial Plastic Surgery & Aesthetic Medicine.ahead of print

Botox and Fillers and Breastfeeding
There is no published research that I have been able to find and trust on the passage of fillers into milk so I cant say that they are safe or unsafe. I just do not know.
There is some information from one mother who caught botulism from eating fermented salmon eggs. She continued to breastfeed. No botulinum toxin or botulism was found in the breastmilk or the baby. The doses that are used medically are far lower than that which would have caused the mother’s botulism so the amount in breastmilk is assumed to be too low to produce adverse effects.
In February 2024 a study of 4 mothers was published https://www.liebertpub.com/doi/abs/10.1089/fpsam.2023.0326
Objective: To detect the presence of botulinum toxin in breast milk from lactating subjects treated with facial botulinum toxin injections, as measured by enzyme-linked immunosorbent assay (ELISA).
Methods: For this pilot study, lactating women were injected with standardized facial botulinum toxin type A (BTXA) (range 40–92 U). Collected breast milk samples over 5 days were analyzed for the presence of botulinum toxin. Exclusion criteria included (1) lactating women still using their breast milk for their infant, (2) muscular disorders, (3) any medication that could interfere with neuromuscular function, (4) uncontrolled systemic disease, (5) pregnant, and (6) neuromodulator injection in the past 90 days.
Results: Four lactating women were recruited. Eight samples had no BTXA detected, whereas 8 of the 16 total had detectable amounts, which were well below the reported lethal oral dose for an infant.
Conclusion of the authors: Although the exclusion of lactating women from receiving cosmetic botulinum toxin injections is out of an abundance of caution to the theoretical risk to the infant, this study helps support the notion that facial botulinum toxin injections do not warrant an interruption in breastfeeding. Further studies with larger sample sizes are needed.
Caroline Hudson, Parker Wilson, David Lieberman, Harry Mittelman, and Sachin Parikh.Analysis of Breast Milk Samples in Lactating Women After Undergoing Botulinum Toxin Injections for Facial Rejuvenation: A Pilot Study.Facial Plastic Surgery & Aesthetic Medicine.ahead of print
References
1. Lee KC, Korgavkar K, Dufresne RGJ et al. Safety of cosmetic dermatologic procedures during pregnancy. Dermatol Surg. 2013;39:1573-86.
2. Middaugh J. Botulism and breast milk. N Engl J Med. 1978;298:343.
Both these cosmetic procedures have to be undertaken with this limited information in mind. It is your choice .
Dental Health and Breastfeeding
As with most professionals, my own included, dentistry seems to lack education on breastfeeding as part of undergraduate training if questions sent to this page exemplify a wider issue. I have tried to provide information for CPD inline with that written for other healthcare professionals.
I have developed this powerpoint presentation on the pharmacokinetics of drugs which dentists may use or prescribe for CPD information in an effort to break down the barriers of continuation of breastfeeding.
I am happy to answer individual questions or training. Please contact wendy@breastfeeding-and-medication.co.uk
In summary:
- Breastfeeding mothers can have local anaesthetic injections with/without adrenaline and continue to breastfeed as normal
- Breastfeeding mothers can take analgesics for dental pain and continue to breastfeed as normal
- Breastfeeding mothers can have antibiotics and continue to breastfeed as normal
- Breastfeeding mothers can use mouthwashes, gels and liquids for mouth ulcers ( e.g. Anbesol®, Bonjela®, Medijel®, Rinstead®, Iglu®, Orajel®) and fluoride toothpastes e.g. Durophat® and continue to breastfeed as normal
- Breastfeeding mothers can have dental sedation for procedures and continue to breastfeed as normal.
- White fillings: In some parts of the UK white fillings are recommended in pregnancy and lactation following an EU Directive (July 2018) but have to be paid for by the patient rather than being part of free NHS treatment. The information states that “These restrictions on the use of dental amalgam aim to help reduce environmental mercury pollution and are not a result of any safety concerns about amalgam fillings for dental patients.”
https://www.sdcep.org.uk/wp-content/uploads/2018/06/SDCEP-Dental-Amalgam-Information-for-Pregnant-or-Breastfeeding-Patients.pdf
- Tooth Whitening: There appears to be no information available on the use of tooth whitening agents during lactation. Whilst it is unlikely that any significant transfer of the agents used into breastmilk will take place, if it can be delayed until breastfeeding has finished naturally, that would be preferable but there are many questions from mothers about to get married who dont want to wait. Unless the products spill from the bath in which the liquid is placed, resulting in burns to the mother’s mouth absorption into breastmilk is unlikely.
For information on mercury fillings please see the information from InfantRisk December 2023
https://www.infantrisk.com/content/mercury-dental-fillings
Data suggests that maternal exposure to mercury vapor from dental amalgams or restoration is unlikely to have a significant impact on breastfeeding infants.
The established baseline for mercury levels in human breastmilk is set at ≥ 1 mcg/L.15 A comprehensive study examining mercury content in breast milk from mothers with dental amalgams revealed a range of mercury concentrations in human milk samples, spanning from < 0.2 to 6.86 mcg/L, with an average of 0.37 mcg/L.16 Studies have demonstrated transfer of mercury from a mother’s bloodstream to her breastmilk. Intriguingly, mercury levels in commercial formula samples displayed a broader spectrum, varying from 0.4 to 2.5 mcg/L on average, which was actually higher than the findings in the collected breastmilk samples.16
Remember, even if materials from mercury amalgams are orally ingested, elemental mercury is not absorbed from a healthy gastrointestinal tract. If a baby consumes miniscule mercury residues in breastmilk, it is likely that it wouldn’t be absorbed, especially as the baby ages and the GI tract matures.
Conclusion
Breastfeeding with mercury fillings or after dental amalgam restoration is likely safe and the benefits of breastfeeding outweigh the risks. Extra-cautious mothers could choose not to breastfeed for the first three days post-amalgam restoration, but the difference in infant risk will be miniscule.
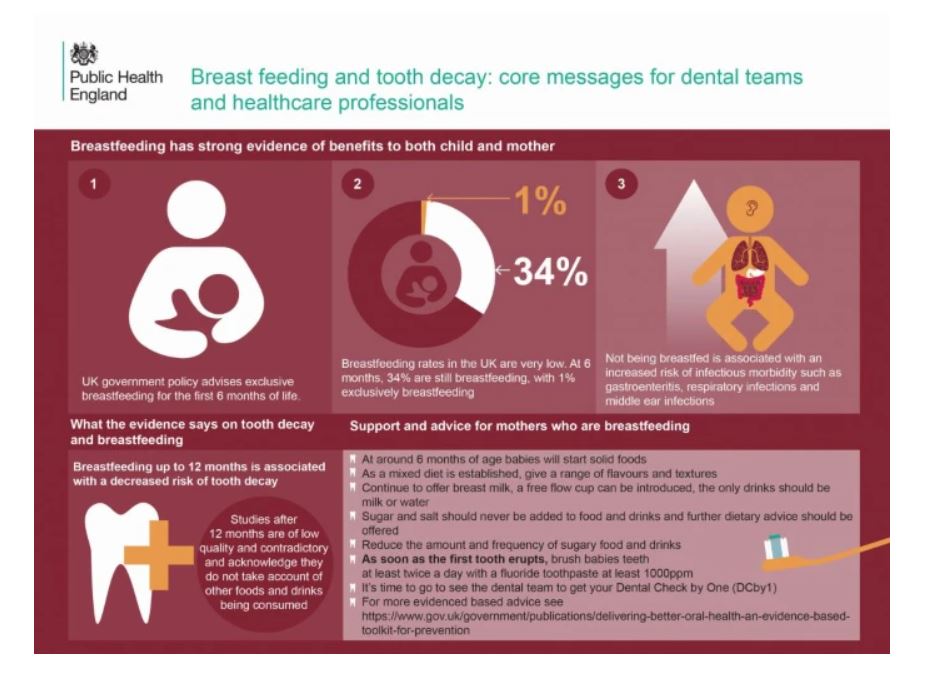
In a report Public Health England have made recommendations on dental health and breastfeeding. Full information can be accessed at : www.gov.uk/government/publications/breastfeeding-and-dental-health/breastfeeding-and-dental-health#breastfeeding-and-dental-health
- dental teams should continue to support and encourage mothers to breastfeed
- not being breastfed is associated with an increased risk of infectious morbidity (for example gastroenteritis, respiratory infections, middle-ear infections)
- breastfeeding up to 12 months of age is associated with a decreased risk of tooth decay
Delivering Better Oral Health (PHE, 2014 updated content 2017)4 recommends that:
- breast milk is the only food or drink babies need for around the first 6 months of their life, first formula milk is the only suitable alternative to breast milk
- bottle-fed babies should be introduced to drinking from a free-flow cup from the age of 6 months and bottle feeding should be discouraged from 12 months old
- only breast or formula milk or cooled, boiled water should be given in bottles
- only milk or water should be drunk between meals and adding sugar to foods or drinks should be avoided
Recent systematic reviews such as that by Tham and others (2015)6 included studies where children were breastfed beyond 12 months. When infants are no longer exclusively breast or formula fed, confounding factors, such as the consumption of potentially cariogenic drinks and foods and tooth brushing practices (with fluoride toothpaste), need to be taken into account when investigating the impact of infant feeding practices on caries development. Tham and others (2015) noted that several of the studies did not consider these factors and concluded that with regard to associations between breastfeeding over 12 months and dental caries “further research with careful control of pertinent confounding factors is needed to elucidate this issue and better inform infant feeding guidelines”. Good quality evidence on breastfeeding and oral health is an area with significant methodological challenges which have been outlined by Peres and others (2018)7.
Of course I would also have to highlight that dental procedures, including sedation, local and general anaesthetic and use of antibiotics and analgesics need not interrupt breastfeeding
Powerpoint training for dental practitioners on passage of drugs in breastmilk
See also:
Prochlorperazine to treat symptoms of labarynthitis/vertigo and Breastfeeding
I am frequently asked about taking prochlorperazine (Buccastem® or Stemetil ®) to treat nausea due to labarynthitis, vertigo or dizziness. It is a drug I would be happy to prescribe and have used it myself as have my breastfeeding daughters. It seems a frequently asked question when the air pressure changes rapidly. Prochlorperazine may also be used for nausea
prochlorperazine and breastfeeding factsheet pdf
Brand names: Stemetil®, Buccastem®
Prochlorperazine is used to treat vertigo, labarynthitis or migraine particularly to treat nauseas caused by these conditions.
Its oral bio-availability is low due to high first-pass metabolism. Long-term use should be avoided in breastfeeding where possible, particularly with very young babies where there is a potential risk of apnoea (breathing problems).
However short-term acute use for vertigo and labarynthitis probably poses few risks. It is widely used for this purpose. It is licensed for use in children over 10 kg.
Compatible with use during breastfeeding if used short term. Avoid long term or where child is at risk of apnoea.
N.B This information is based on anecdote and experience as there are no research based studies on the amount passing into breastmilk.
see also https://breastfeeding-and-medication.co.uk/fact-sheet/betahistine-and-breastfeeding
ADHD and Breastfeeding
I have shared the chapter on ADHD from my book Breastfeeding and Chronic Medical Conditions multiple times this week. Many mothers seem to be diagnosed in later life and are concerned about breastfeeding. Hope this is a useful link.
More information
ADHD and Breastfeeding Factsheet
If this is useful maybe you need the book available on Amazon. I published on Kindle to try to make this more affordable and available to mothers and breastfeeding supporters as well as professionals
I came off my medication to conceive and my baby is now 6 months old. I am really struggling to think straight now and getting really overwhelmed by the smallest of things.
Description
ADHD is a disorder that includes symptoms such as inattentiveness, hyperactivity, and impulsiveness. It is normally diagnosed in childhood, but some parents have found themselves being diagnosed when seeking a diagnosis for their children. The cause is unknown, but it seems to at least in part, genetic. It has been suggested that being born prematurely (before the 37th week of pregnancy), having a low birth weight or maternal smoking or alcohol or drug abuse during pregnancy may be linked. Attention deficit hyperactivity disorder (ADHD) is thought to affect about 1 in 20 children in the UK with incidence being three times higher in boys.
Symptoms fall into 2 categories:
inattentiveness main symptoms of which are:
- having a short attention span and being easily distracted
- making careless mistakes
- appearing forgetful or losing things
- being unable to stick to tasks that are tedious
- appearing to be unable to listen to or carry out instructions
- constantly changing activity or task
- having difficulty organising tasks
hyperactivity and impulsiveness main symptoms of which are:
- being unable to sit still and constantly fidgeting
- being unable to concentrate on tasks
- excessive physical movement
- excessive talking
- being unable to wait turn
- acting without thinking
- interrupting conversations
- little or no sense of danger
- ADHD may be linked with anxiety, autism, and several other conditions. By the age of 25, an estimated 15% of people diagnosed with ADHD as children still have a full range of symptoms, and 65% still have some symptoms that affect their daily lives. ( https://www.nhs.uk/conditions/attention-deficit-hyperactivity-disorder-adhd/symptoms/)
- Treatment
- Methylphenidate (Ritalin ™, Concerta ™); works by increasing the amount of a dopamine in the parts of the brain responsible for self-control and attention. It is usually the first line treatment. There are side effects of loss of appetite and difficulty sleeping and mood swings. Limited evidence indicates that methylphenidate levels in milk are very low and not detectable in infant serum. The effects of methylphenidate in milk on the neurological development of the infant have not been well studied. Monitor the baby for agitation, irritability, poor sleeping patterns, changes in feeding and poor weight gain.
- Atomexatine is a selective noradrenaline reuptake inhibitor (SNRI), increasing levels of noradrenaline rather than dopamine. It can aid concentration and help control impulses. Side effects include rise in blood pressure and heart rate, nausea and vomiting, gastric pain, difficulty sleeping, dizziness, headaches, and irritability. More importantly it has been associated with suicidal thoughts and liver damage. There is no published experience with atomoxetine during breastfeeding, although reports from the manufacturer found no serious adverse effects in two breastfed infants (Besag 2014).
- Dexamphetamine. Side effects include decreased appetite, mood swings, agitation and aggression, dizziness, headaches, nausea, vomiting and diarrhoea. Only used if lisdexamphetamine is helpful but not tolerated. In dosages prescribed for medical indications, some evidence indicates that dextroamphetamine might not affect nursing infants adversely. The effect of dextroamphetamine in milk on the neurological development of the infant has not been well studied. It is possible that large dosages of dextroamphetamine might interfere with milk production. Infant Monitoring for agitation, hyperactivity, insomnia, decreased appetite, weight gain, and tremor.
- Lisdexamphetamine (Vyvance ™) may be offered as first line treatment in adults. Side effects include decreased appetite, aggression or drowsiness, dizziness, headaches, nausea, vomiting and diarrhoea. Lisdexamfetamine is a prodrug of dextroamphetamine. In medicinal dosages, some evidence (5 mothers studied) indicates that dextroamphetamine might not affect nursing infants adversely. The effect of dextroamphetamine in milk on the neurological development of the infant has not been well studied. Infant Monitoring should be for agitation, irritability, poor sleeping patterns and poor weight gain.
- The NHS website suggests that for adults with ADHD if you find it hard to stay organised, then make lists, keep diaries, stick up reminders and set aside some time to plan what you need to do
- let off steam by exercising regularly
- find ways to help you relax, such as listening to music or learning relaxation techniques
- if you have a job, speak to your employer about your condition, and discuss anything they can do to help you work better
- talk to your doctor about your suitability to drive, as you will need to tell the Driver and Vehicle Licensing Agency (DVLA) if your ADHD affects your driving
- contact or join a local or national support group – these organisations can put you in touch with other people in a similar situation, and can be a good source of support, information, and advice
References
- Attention deficit hyperactivity disorder: diagnosis and management; NICE guideline (March 2018, updated September 2019)
- Attention deficit hyperactivity disorder; NICE CKS, May 2018
- Besag FM. ADHD treatment and pregnancy. Drug Saf. 2014; 37:397-40
- NHS ADHD https://www.nhs.uk/conditions/attention-deficit-hyperactivity-disorder-adhd/living-with/
- Further Information
- AADUK https://aadduk.org/
Low dose aspirin and breastfeeding
It is not uncommon for breastfeeding mothers to need to take low dose aspirin, sometimes for reasons in pregnancy or after cardiac events. Whilst it isnt recommended regularly as a painkiller at a dose of 600mg four times a day it is compatible with breastfeeding in low dose of 75-150mg daily. There are no reported cases of Reye syndrome associated with the amount of low dose aspirin passing through breastmilk and it is widely used, particularly during pregnancy.
low dose aspirin and breastfeeding pdf
If accidentally taken at an analgesic dose see https://breastfeeding-and-medication.co.uk/fact-sheet/accidentally-taking-one-dose-of-aspirin-when-breastfeeding
Aspirin 75 -150mg acts by decreasing platelet adhesiveness irreversibly inhibiting aggregation. It is not used during treatment of thrombosis but may be used in cases of recurrent miscarriage or with risk of pre-eclampsia. In more serious conditions it is used post myocardial infarction (MI) and stroke or to decrease cardiovascular risk. There is little evidence that enteric-coated tablets are less likely to increase the risk of GI bleeds and may be less effective in their anti-platelet activity as well as more expensive. Although aspirin is not recommended during breastfeeding at analgesic doses of 600 mg four times a day, due to its association with Reye’s syndrome, use of the small dose in these circumstances may be considered to be acceptable. In the absence of the risk of association of Reye’s syndrome, aspirin would be a drug compatible with lactation due to its pharmacokinetic properties.
Before the link with Reye’s syndrome was identified, the children’s dose of aspirin was 75 mg four times a day. Relative infant dose is quoted as 2.5–10.8% (Hale 2017 online access). The BNF states that it should be avoided due to possible risk of Reye’s syndrome. Regular use of high doses could impair platelet function and produce hypo-prothrombinaemia in infant if neonatal vitamin K stores are low. After 2-4 hours there is virtually no aspirin in milk Compatible with breastfeeding if necessary at 75 -150mg mg daily, avoid as an analgesic Reye’s syndrome This is a rare syndrome, characterized by acute encephalopathy and fatty degeneration of the liver, usually after a viral illness or chickenpox. The incidence is falling but sporadic cases are still reported. It was often associated with the use of aspirin during the prodromal illness. Few cases occur in white children under 1 year although it is more common in black infants in this age group. Many children retrospectively examined show an underlying inborn error of metabolism.
High Dose Vitamin D Supplements and Breastfeeding
The question as to the compatibility of high dose vitamin d supplements in the breastfeeding mother is a frequently asked question. We appear to monitor levels more frequently than we did in the past but research is difficult to source. I hope this information helps.
pdf of this information.
High dose vitamin d supplement for breastfeeding mothers factsheet

There has been an unexpected increase over the past 15 years in the number of babies found to be suffering from rickets or symptoms of decreased bone mass which demonstrate poor levels of vitamin D (NICE PH11). Vitamin D deficiency is unusual in babies born at term to mothers with adequate vitamin D status. Some women enter pregnancy with low vitamin D levels. This may be due to:
• lack of exposure to sunlight due to wearing concealing clothing for cultural reasons;
• inadequate consumption of foods containing vitamin D e.g. oily fish;
• Inadequate consumption of dairy (prevalent particularly in adolescent girls)
• BMI greater than 30;
• Women who spend a lot of time indoors or use sun creams limiting the absorption of ultraviolet (UV) light;
• living in the northern hemisphere where levels of UV light are only sufficient to stimulate vitamin D production in the summer months; and
• having dark skin, which prevents absorption of available UV light in the UK climate.
Babies born to mothers with low vitamin D levels may be born deficient. In turn this will be exacerbated by being breastfed as the vitamin D levels in breastmilk will be sub-optimal.
In 2016 SACN amended recommendations so that breastfed babies from birth to one year of age should be given a daily supplement containing 8.5 to 10mcg of vitamin D as a precaution and breastfeeding mothers should also take a daily Vitamin D supplement of 10 µg (400IU) per day
This in no way suggests that the breastmilk of a mother with low levels of vitamin D, does not have all the other health advantages but is a reflection of current awareness of the risk of sun damage in sunlight balanced with the UK climate and poor levels of sunshine for the majority of the year. Breastfeeding alone cannot redress the deficiency resulting from low levels in pregnancy. Vitamin D is a fat-soluble vitamin that is found in food and can also be made in the body after exposure to UV rays from the sun. Fortified foods are common sources of vitamin D but without sunshine exposure it is difficult to achieve maximal intake. Supplements can be taken as part of multi-vitamin products or with calcium.
Sources of vitamin D
• More than 90% of mankind’s vitamin D supply is derived from UVB sunlight exposure
• Oily fish including trout, salmon, mackerel, herring, sardines, anchovies, pilchards and fresh tuna
• Cod liver oil and other fish oils
• Egg yolk – 0.5 µg (20 IU) per yolk
• Mushrooms
• Supplemented breakfast cereals, mainly supermarket ‘own brands’ in the UK. Typically contain between 2 and 8 µg (80-320 IU) per 100 g
• Margarine
In a fair-skinned individual, exposure of the face and forearms to 20–30 minutes of sunlight at midday is estimated to generate the equivalent of 2000 IU vitamin D. Between April and October all of Scandinavia, much of western Europe, including 90% of the UK (roughly north of Birmingham) and 50% of USA is above the latitude where exposure to sufficient UVB is possible (Pearce 2010).
High dose vitamin d supplements
Many breastfeeding mothers appear to be being diagnosed as vitamin D deficient and prescribed high doses daily or weekly. Hollis et al 2015 reported that “Maternal vitamin D supplementation with 6400 IU/day safely supplies breast milk with adequate vitamin D to satisfy her nursing infant’s requirement and offers an alternate strategy to direct infant supplementation. With the use of higher dose supplements the mother should observe the baby for signs of hyper calcaemia (nausea, vomiting, weight loss, thirst, muscle weakness and confusion) and if observed blood test the baby.
Hollis and Wagner (2004) studied 18 women exclusively breastfeeding one month after delivery, and gave half 1600 IU vitamin D2 and 400 IU vitamin D3 and the others 3600 IU vitamin D2 and 400 IU vitamin D for 3 months. Blood, urine, and milk samples were obtained from the mothers at months 1, 2, 3, and 4 of lactation. Infant blood was collected at months 1 and 4 (beginning and end of the study). Maternal blood was monitored for total calcium, vitamin D2, vitamin D3, 25(OH)D2, and 25(OH)D3 concentrations. Infant serum was monitored for vitamin D2, vitamin D3, 25(OH)D2, 25(OH)D3, calcium, and phosphorus concentrations. The conclusion of the study was that the 400iu per day has been recommended arbitrarily and needs further research. In the study maternal vitamin D intakes of ≥4000 IU/d appear to be safe and to provide sufficient vitamin D to ensure adequate nutritional vitamin D status for both mothers and nursing infants.
- Hollis BW, Wagner CL, Vitamin D requirements during lactation: high-dose maternal supplementation as therapy to prevent hypovitaminosis D for both the mother and the nursing infant, Am J Clin Nutr, 2004;80(6 Suppl.):1752S–8S. (https://academic.oup.com/ajcn/article/80/6/1752S/4690524)
Hollis et al (2015) randomised 3 groups of exclusively breastfeeding women to 400 IU vitamin D3 per day 2400 IU or 6400 IU vitamin D3 per day, The infants of the mothers in group one were given a vitamin d supplement but those in the higher dose groups received placebo drops. 148 mothers completed the full study still exclusively breastfeeding. The conclusion of the study was that maternal vitamin D supplementation with 6400 IU/day safely supplies breast milk with adequate vitamin D to satisfy her nursing infant’s requirement and offers an alternate strategy to direct infant supplementation. This was not achieved with lower doses.
- Hollis BW, Wagner CL, Howard CR, Ebeling M, Shary JR, Smith PG,Taylor SN, Morella K, Lawrence RA,Hulsey TC, Maternal Versus Infant Vitamin D Supplementation During Lactation: A Randomized Controlled Trial. Pediatrics 2015;136 (4): 625-634 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4586731/pdf/peds.2015-1669.pdf
Some mothers are prescribed 20,000 or 40,000 units once weekly which approximate to a similar dosage. There is limited research to support this level being compatible with breastfeeding so the baby should be monitored for hypercalcaemia as described above – nausea, vomiting, weight loss, thirst, muscle weakness and confusion
See also: https://www.ncbi.nlm.nih.gov/books/NBK500914/
https://www.sps.nhs.uk/articles/using-vitamin-d-during-breastfeeding (December 2023)
For full references see Breastfeeding and Medication 2018
Opioids and breastfeeding
When paracetamol plus a non steroidal drug (ibuprofen, naproxen, diclofenac or celecoxib) are insufficient to control pain opioid drugs may need to be used. They cause constipation so should be co prescribed with a stool softener). They are also addictive so should be used for the shortest possible time, in the lowest possible dose.
Codeine is not recomemnded for breastfeeding https://breastfeeding-and-medication.co.uk/thoughts/breastfeeding-and-codeine but one accidental dose or short term use, maybe overnight when no other pain relief is available does not mean that breastfeeding needs to be interrupted.
No breastfeeding mother should ever be asked to choose between adequate pain relief and breastfeeding
Opioids and breastfeeding factsheet
Mirtazapine and breastfeeding
Another medication used during breastfeeding for anxiety and depression is mirtazapine. It may be used where other SSRIs have not been effective or tolerated. Mirtazapine may be also be seen as an option where insomnia is a symptom of anxiety or depression.
The baby should be observed for signs of drowsiness and ineffective feeding.
Care should be taken with co sleeping because it is likely to cause drowsiness in the lactating mother. Falling asleep in chairs or on sofas should be regarded as an even greater risk https://www.basisonline.org.uk/
LactMed summarises that “Limited information indicates that maternal doses of up to 120 mg daily produce low levels in milk and would not be expected to cause any adverse effects in breastfed infants, especially if the infant is older than 2 months.” In practice the normal dose is 15mg taken at night.
Professionals may find the RCGP Perinatal mental health toolkit a useful resource https://www.rcgp.org.uk/clinical-and-research/resources/toolkits/perinatal-mental-health-toolkit.aspx
The information in this factsheet is taken from my book Breastfeeding and Medication. Please message me with queries or the references used. wendy@breastfeeding-and-medication.co.uk
Mirtazapine and Breastfeeding Factsheet