Home » Articles posted by Wendy Jones (Page 3)
Author Archives: Wendy Jones
Nausea and Breastfeeding
One of the more frequently asked questions recently relates to nausea and even vomiting when breastfeeding. It may be due to norovirus, pregnancy (see https://breastfeeding-and-medication.co.uk/fact-sheet/vomiting-in-pregnancy-whilst-still-breastfeeding ) or to stop nausea from medication e.g morphine.
I hope this factsheet provides some options. The information is taken from my book Breastfeeding and Medication which provides more details and references. Maybe you need to buy a copy?
Nausea can be triggered by a variety of factors including food poisoning, motion sickness, labarynthitis, vertigo, pregnancy, migraine or as a symptom of other underlying conditions.
Cinnarazine (Stugeron®)
Cinnarazine is used for symptomatic treatment of nausea and vertigo caused by Ménière’s disease as well as prevention of travel sickness. There are no data on transfer into breastmilk but it is licensed for use in children.
Probably compatible with use during breastfeeding. Although there are no data on transfer into breastmilk, it is licensed for use in children.
Prochlorperazine ( Stemetil®, Buccastem®)
Prochlorperazine is used to treat vertigo, labarynthitis, migraine or drug-induced emesis. Its oral bio-availability is low due to high first-pass metabolism. Long-term use should be avoided in breastfeeding where possible, particularly with very young babies where there is a potential risk of apnoea. However short-term acute use probably poses few risks as it is licensed for use in children over 10 kg.
Compatible with use during breastfeeding if used short term. Avoid long term or where child is at risk of apnoea.
Domperidone (Motilium®)
Domperidone stimulates gastric emptying. It causes fewer central effects such as sedation and dystonia (although there are still reports of these) because it does not cross the blood–brain barrier. Its dopamine antagonist activity stimulates prolactin release, which makes it useful as a galactagogue.
Domperidone is metabolised by cytochrome P450 so care should be taken with potential interactions. It is more than 90% bound to plasma proteins and has a low bio-availability on an empty stomach (15%) when taking orally due to first-pass hepatic and intestinal metabolism.
Doses of more than 60 mg per day have been associated with sudden cardiac death although reports have been predominantly in the elderly and in those receiving intravenous doses (FDA 2004, Joss et al. 1982, Giaccone et al. 1984, Weaving 1984, Roussak 1984, Osborne et al. 1985, manufacturers information 2012).
Compatible with use during breastfeeding due to extensive plasma protein binding. See also information as a galactogogues.
Metoclopramide (Maxolon®, Migravess®, Paramax®)
Metoclopramide is a dopamine antagonist and can cause extra-pyramidal side effects, in particular, acute dystonia. This adverse effect is most commonly seen in children and young adults, especially females, so it is not a drug of choice in lactating mothers who generally fall into this age group. It may also precipitate hypotension and depression. Other side effects reported include headache, diarrhoea, dry mouth and change in appetite (Ingram et al. 2011). It stimulates prolactin secretion and has been used as a galactogogue but has now been superseded. The bio-availability of oral metoclopramide is about 75% but varies widely between patients due to its hepatic first-pass metabolism. Concentrations higher than those in maternal plasma may be reached in breastmilk particularly in the early puerperium, although these decrease with increased maturity.
Compatible with use during breastfeeding but avoid if possible due to risk of extrapyramidal effects and link with depression. Use domperidone as an alternative.
Cyclizine (Valoid®)
Cyclizine is an anti-emetic used to treat motion sickness, post-operative nausea and vomiting, after radiotherapy, and in drug- induced situations as well as nausea in pregnancy. There are no reports of levels entering breastmilk (BNF) or data on which to base conclusions. There is an unlicensed dose for children aged over 6 years.
Avoid if possible as no information on passage into breastmilk although if use considered essential unlikely to produce adverse effects if used short term. Longterm use may cause drowsiness in baby and consequent weight loss.
Hyoscine (Joy Rides®, Kwells®)
Hyoscine produces a reduction in salivation as well as some sedation. It is commonly used to prevent travel sickness as well as other types of nausea, either as an oral tablet or as a patch. It is believed to pass into breastmilk but no studies report the amounts. No reports of adverse effects appear to have been made and it appears compatible with breastfeeding, particularly to prevent travel sickness. Long-term use could decrease lactation.
BNF suggests that the amount in breastmilk is too small to be harmful.
Safe to use during breastfeeding to prevent travel sickness. No studies on passage into breastmilk but no adverse events reported so safety presumed as used in paediatric doses.
Ondansetron ( Zofran®)
This drug is a 5-HT3 antagonist with antiemetic activity. It is used in the management of nausea and vomiting induced by cytotoxic chemotherapy and radiotherapy. It is also used for the prevention and treatment of post-operative nausea and vomiting that have not responded to other antiemetic agents. Ondansetron may also be used for nausea in pregnancy. It is licensed for use in children from two years of age. It is 60% orally bio-available and 70–75% plasma protein bound. The terminal half-life is 3 hours after oral doses. There are no studies on transfer into breastmilk although it has been found in animal studies (BNF).
Avoid if possible as no information on passage into breastmilk but licensed for use in children > 2 years.
See also https://www.sps.nhs.uk/articles/treating-nausea-during-breastfeeding

Hypertension (raised blood pressure) and Breastfeeding
Many mothers experience raised blood pressure it seems. Is this due to our busy lifestyles, more mums giving birth at an older age? Who knows but it causes a lot of confusion. The drug normally initiated if a mother has symptoms of pre-eclampsia is labetolol. It is usually continued after delivery until the BP has settled. Virtually none passes into breastmilk. However, some mothers with poor circulation may notice sore, white nipples where the supply to the tip is decreased . If this happens the drug may need to be changed. Prolonged high BP in pregnancy can lead to restricted growth of the baby who may be born sleepy. Rather than just monitoring blood glucose levels the baby should be helped to attach to the breast and feed regularly or be given colostrum by spoon or syringe. A drop of colostrum can work magic.
Later blood pressure rises can be treated with enalapril, amlodipine and felodipine which are all compatible with breastfeeding according to expert sources. The NICE Guidelines NG 133 (2019) can also guide good practice.
The data for this fact sheet is taken from my book Breastfeeding and Medication which provides more detail and references to studies. Please consider buying a copy for future reference.
There is much information in this factsheet.
Hypertension (raised blood pressure) is defined as sustained blood pressure above 140/90. Diet, obesity, heredity, race and stress all impact on blood pressure. High cholesterol, high salt content in the diet and saturated fat intake increases the long-term health risk.
Breastfeeding women may have had a previous event which presents a challenge to pregnancy and lactation e.g., stroke, heart attack, renal complications, SVT etc. In the past these might have produced barriers to childbirth but now seem to be so well controlled mothers are able to give birth and look after their own health.
There are several types of drugs used to treat hypertension some of which we have no data on with respect to use in breastfeeding mother, others should be avoided where possible.
For more details and references see Breastfeeding and Medication Jones W Routledge 2018
Diuretics
All diuretics should be avoided unless essential for health of the mother. By removing excess fluid from the body diuretics may reduce milk supply. This is more likely with furosemide than Bendroflumethiazide or bumetanide, but this category of drugs should be avoided during lactation to control blood pressure but only fluid retention, where essential
Bendroflumethiazide – unknown effect from low dose 2.5mg daily
Indapamide – No information is available on the amount of indapamide in breastmilk. Intense diuresis with large doses may decrease breastmilk production.
Furosemide – more likely to reduce supply due to intense diuresis
Bumetanide – low risk in established supply
Spironolactone – an aldosterone receptor antagonist used as a diuretic in various conditions associated with oedema, as well as in the treatment of hypertension. Its value is in sparing potassium loss. It is metabolised to canrenone which was found in the breastmilk of one mother taking 25mg four times a day by Phelps (1977). He suggested the amount absorbed by the baby would be 0.2% of the mother’s daily dose. Spironolactone is 90% plasma protein bound and has a bioavailability of 90% (Martindale 2017) 70% (Hale 2017). The American Academy of Paediatrics considers it compatible with breastfeeding. The BNF states that although its metabolite is present in milk, the amount is probably too small to be harmful.
ACE inhibitors
This family of drugs are potentially teratogenic but can be used during lactation
Enalapril. This is the ACE with most evidence of safety during lactation. Redman et al. (1990) studied five women taking 20 mg enalapril, it was not detectable after 4 hours in four of the five women while the average peak level of enalaprilat (the metabolite of enalapril) was 1.7 µg per litre. No adverse events were reported in four babies exposed to maternal levels of 5–10 mg. Huttenen et al. (1989) studied three women after single doses of enalapril up to 10 mg. Enalaprilat levels were not detected and the concentration of ACE activity in milk was unchanged. Rush et al. (1989) deduced that the total amount of enalapril and its metabolite to which a baby would be exposed was 2 µg of enalaprat while unlicensed use of enalapril from 1 month (BNFC) is 100 µg per kilogramme per day. Relative infant dose quoted as 0.2% (Hale 2017 online access).
BNF data recommend that the drug is avoided in the first few weeks after delivery due to the risk of profound neonatal hypotension; it can be used in older infants if essential but recommends that the infant’s blood pressure is monitored.
Compatible with breastfeeding. Amount transferred into breastmilk is significantly less than can be given directly to a baby more than 1 month of age.
Captopril: Devlin and Fleiss’ study (1981) of 12 women showed that the concentration of captopril in breastmilk was about 1% of maternal plasma, equivalent to 4.7 µg per litre in breastmilk of mothers taking 300 mg daily and no adverse effects were noted in the babies. Compatible with breastfeeding. Amount transferred into breastmilk is significantly less than can be given directly to a baby more than 1 month of age.
Ramipril: No data are available on transfer into breastmilk. Ramipril has an active metabolite ramiprilat, which is approximately 56% plasma protein bound.
Lisinopril: There is no information on the transfer of lisinopril into breastmilk, although the oral bioavailability is only 29%. It is not significantly bound to plasma proteins.
Perindopril: There are no data available on the transfer of perindopril into breastmilk. It is metabolised to perindoprilat which is the active drug. Plasma protein binding is reported to be 10–20% and oral bioavailability is 65–75%.
Quinapril: rapidly converted to its active metabolite quinaprilat. Begg studied 6 women taking 20mg quinapril daily. Four hours after the dose no drug was recovered from milk. No Quinaprilat was detected at any time. The authors therefor suggested that quinapril is safe in breastfeeding.
Beta blockers
Beta blocker of choice in a mother during breastfeeding based on evidence of benefit and safety for the baby is Metoprolol, propranolol or labetolol
In many maternity units the use of beta blockers triggers the hypoglycaemia policy involving blood sugar testing. The amount of labetolol, propranolol and metoprolol passing into breastmilk is low and these drugs are less likely to lower blood sugars than atenolol (which has low plasma protein binding and passes more extensively into milk). The risk to the baby stems from the fact that babies born to mothers with pre-eclampsia may be born (or induced) early or may have experienced intra-uterine growth retardation. The efficacy of the baby’s feeding and milk transfer should be assessed as well as blood sugars. If necessary, the mother may need to hand express and syringe/cup/spoon feed colostrum to her infant.
Atenolol: diffuses into breastmilk in concentrations similar to or higher than those in maternal blood demonstrated by m/p ratios of 1.5–6.8. Despite this, the authors calculated the infant would only be exposed to 0.13 mg per day following a maternal dose of 50 mg per day (Liedholm 1983). Cyanosis and bradycardia in a 5-day-old term infant associated with maternal intake of 50 mg atenolol twice daily in breastmilk has been reported. The infant recovered when breastfeeding was interrupted (Schimmel et al. 1989). Other authors have reported no adverse effects in 15 infants aged 3 days to 2 weeks exposed to 50–100 mg atenolol (Bhamra et al. 1983; White et al. 1984; Kulas et al. 1984). It is not licensed for use in children under the age of 12 years. Relative infant dose quoted as 6.6% (Hale 2017 online access).
Atenolol has low plasma protein binding and therefore passes more freely into breastmilk. Caution is particularly advised in neonates because of the renal excretion of this drug.
Labetolol; Michael’s study of 25 patients (1979) taking between 330 and 800 mg labetolol daily showed a m/p ratio less than 1, although one patient taking 1200 mg daily produced milk samples where the concentration in milk exceeded that in maternal plasma. Lunell et al.’s study (1985) produced similar results. However, no baby in these studies exhibited any adverse drug reactions. Mirpuri et al. (2008) reported that a 26-week premature baby exhibited bradycardia and premature beats when tube fed expressed breastmilk from its mother who was receiving 300 mg labetolol twice daily. Its condition returned to normal when formula milk was substituted. McGuinness identified that a mother’s intake of labetolol had triggered symptoms of Raynaud’s syndrome due to restriction of blood flow to the extremities. This should be borne in mind with any mum reporting panful breastfeeding when on beta blockers.
Metoprolol: Studies have shown that metoprolol also produces m/p ratios in excess of 1 (Sandström and Regårdh 1980; Liedholm et al. 1981). However, the absolute level of drug transferring to the baby is small and studies have failed to detect metoprolol at significant levels in infant plasma (Kuklas et al. 1984). Although the drug is well-absorbed, it undergoes extensive first-pass metabolism. No adverse events have been reported in babies exposed to metoprolol via breastmilk (Ho et al. 1999; Lindeberg et al. 1984
Bisoprolol: Only one study of the use of bisoprolol appears in the literature. Khurana studied a mother who was initiated on it 6 days after birth for a cardiac condition. She expressed samples of milk on day 11 and 18 after birth. Drug levels in milk were undetectable but the baby did not receive any breastmilk, so data is incomplete. See https://breastfeeding-and-medication.co.uk/fact-sheet/bisoprolol-and-breastfeeding
Propranolol: almost completely absorbed from the gastrointestinal tract but undergoes first-pass metabolism. It is highly lipid soluble and is approximately 90% plasma protein bound. It has at least one active metabolite but the impact of this is unclear.
In adults it may be used to lower blood pressure, to relieve symptoms of hyperthyroidism, to prevent migraines or to prevent panic attacks. See https://breastfeeding-and-medication.co.uk/thoughts/propranolol-and-breastfeeding
In a study of three women (Smith 1983) it was calculated that the maximum dose likely to be ingested by a breastfed infant would be less than 0.1% of the maternal dose.
Angiotensin II receptor antagonists
This group of drugs is given to patients who are unable to tolerate ACE inhibitors to treat hypertension and heart failure. As with ACE inhibitors, this group of drugs is contra-indicated in pregnancy. There are few data on transfer into breastmilk and the use of ACE inhibitors is recommended. This class of drug might be expected to produce low levels in breastmilk because of the high protein binding and low bioavailability but no data exist to support this assumption.
Candestartan : has limited oral bio availability of 14%, and a plasma protein binding > 99%. There is one study of 3 breastfeeding mothers, all stabilized on candesartan (8-32 mg daily ). They provided milk and plasma samples over 24 hours. Plasma samples were obtained from 2 of the babies The relative infant dose was estimated to be 0.09%. Candesartan was undetectable (less than 0.2 micrograms/L) in infant plasma samples (Coberger 2019, LactMed).
Irbesartan; oral bio availability 60-80% and plasma protein binding 90%. Because no information is available on the use of irbesartan during breastfeeding it is best avoided. If a sartan is considered essential candesartan might be preferable
Losartan; oral bio availability of 33%, and high plasma protein binding of 99.8%. Kearney (2018) suggests that the high protein-binding of losartan and low oral bioavailability makes excretion into breast milk and subsequent absorption by the baby unlikely. She suggests that if the mother has developed Postpartum cardiomyopathy, breastfeeding need not be discouraged. However, there are no relevant published data on excretion into breast milk.
Valsartan; has an oral bio availability 23%, and plasma protein binding of 95%. There are no relevant published data on excretion into breast milk. Candesartan may be seen as the best option if a sartan is considered essential.
Calcium channel blockers
Nifedipine: relaxes vascular smooth muscle and dilates coronary and peripheral arteries. It has activity in reducing blood pressure and in the treatment of Reynaud’s syndrome. Nifedipine is almost completely absorbed from the GI tract but undergoes extensive first-pass metabolism. Side effects for the mother include flushing and headache, which may limit its usefulness. It is present in breastmilk but in levels too small to be harmful and there have been no reports of adverse effects in babies. See https://breastfeeding-and-medication.co.uk/fact-sheet/february-is-raynaud-s-awareness-month-www-sruk-co-uk
Amlodipine: A study of 31 postpartum women (Naito 2015) with pregnancy-induced hypertension received amlodipine 5 mg daily by mouth, with the dosage increased as needed to maintain blood pressure of 140/90 mm Hg or less (mean dosage for the group was 6 mg daily. Maternal blood and breastmilk samples were obtained after at least 6 days of therapy. The median milk concentration was 11.5 µg/L, and no infant showed any adverse effects.
Felodipine: Small amounts of felodipine may get into breast milk, but it’s not known if this is harmful to the baby (BNF). Oral bio availability 20%, plasma protein binding >99%, no studies of passage into breastmilk have been located
Diltiazem: Diltiazem is used for its antiarrhythmic, anti-anginal and antihypertensive properties but rarely in women of childbearing age unless there are very specific indications from the medical history. It is rarely used simply to treat hypertension.
Alpha blockers
Avoid unless essential to mother’s health. This class of drugs are generally only used in addition to other drugs with poorly controlled blood pressure. They are not normally used as first line or monotherapy
Doxazosin: Jensen published a paper on one mother breastfeeding a 6-month-old. She received 4 mg daily for 2 days. The maximum milk concentrations were 2.9 and 4.2 µg/L. This drug should only be used in extreme circumstances and with close monitoring of the infant, for drowsiness, poor feeding, low blood pressure.
Terazosin: no studies in breastfeeding. Terazosin has rather powerful effects on the prostate and testes producing testicular atrophy in some animal studies (particularly new-born) and is therefore not preferred in pregnant or in lactating women (Hale)
NICE Guidance NG 133 (June 2019)
1.9 Antihypertensive treatment during the postnatal period, including during breastfeeding
1.9.1 Advise women with hypertension who wish to breastfeed that their treatment can be adapted to accommodate breastfeeding, and that the need to take antihypertensive medication does not prevent them from breastfeeding. [2019]
1.9.2 Explain to women with hypertension who wish to breastfeed that:
- antihypertensive medicines can pass into breast milk
- most antihypertensive medicines taken while breastfeeding only lead to very low levels in breast milk, so the amounts taken in by babies are very small and would be unlikely to have any clinical effect
- most medicines are not tested in pregnant or breastfeeding women, so disclaimers in the manufacturer’s information are not because of any specific safety concerns or evidence of harm.
- Make decisions on treatment together with the woman, based on her preferences. [2019]
1.9.3 As antihypertensive agents have the potential to transfer into breast milk:
- consider monitoring the blood pressure of babies, especially those born preterm, who have symptoms of low blood pressure for the first few weeks
- when discharged home, advise women to monitor their babies for drowsiness, lethargy, pallor, cold peripheries or poor feeding. [2019]
1.9.4 Offer enalapril [5]to treat hypertension in women during the postnatal period, with appropriate monitoring of maternal renal function and maternal serum potassium. [2019]
1.9.5 For women of black African or Caribbean family origin with hypertension during the postnatal period, consider antihypertensive treatment with: nifedipine [3] or amlodipine if the woman has previously used this to successfully control her blood pressure. [2019]
1.9.6 For women with hypertension in the postnatal period, if blood pressure is not controlled with a single medicine, consider a combination of nifedipine [3] (or amlodipine) and enalapril [5]. If this combination is not tolerated or is ineffective, consider either: adding atenolol or labetalol to the combination treatment or swapping 1 of the medicines already being used for atenolol or labetalol. [2019]
1.9.7 When treating women with antihypertensive medication during the postnatal period, use medicines that are taken once daily when possible. [2019]
1.9.8 Where possible, avoid using diuretics or angiotensin receptor blockers [5] to treat hypertension in women in the postnatal period who are breastfeeding or expressing milk. [2010, amended 2019]
1.9.9 Treat women with hypertension in the postnatal period who are not breastfeeding and who are not planning to breastfeed in line with the NICE guideline on hypertension in adults. [2019]
Inflammatory Bowel Disease and Breastfeeding
Many people know that I have had Crohns disease since I was 22 years old – that was when it was officially diagnosed but probably from 4 years before when I was 18 years old. It has had an immense effect on my life firstly medically – I have had 3 bowel resections and been on medications since the last one in 2002 which very nearly killed me. The only times when I was really fit in and well were when I was pregnant and breastfeeding which sparked my interest in becoming a breastfeeding counsellor 35 years ago. It meant I fed my second and third daughters for much longer (I became very ill soon after I weaned my first) and became passionate about supporting women to breastfeed. As a pharmacist that rolled into an interest and then passion about drugs in breastmilk.
When I regularly had contact with mums with IBD asking about their medication I decided to set up the Facebook group as a mutual support group. Mums who understood the urgency of toilet visits when out shopping, understood how debilitating it was to be in constant pain, that we could discuss anything in a private forum with others in the same situation. Coincidentally it has become a place where people ask each other about drugs and look to me to provide evidence of safety in breastfeeding – that wasn’t the original intent but an excellent spin off.
I havent set up any other specialist interest groups – this is out of my personal interest. Unsurprisingly the diagnosis and treatment of inflammatory bowel disease has taken up a lot of space in my book Breastfeeding and Medication and I am keen that professionals understand that breastfeeding protects our babies but is also something which we value above many things.
As of this morning we have 1.6K members from all over the world, climbing steeply recently January 2022).
Specialists seem to be very concerned about the safety of the drugs – which are strong admittedly and breastfeeding. But we also need to bear in mind that IBD is at least partly linked with being formula fed so we want to maintain breastfeeding and use specialist sources.
Live vaccines may be delayed or omitted – particularly the rotavirus vacc. However, this is as much to protect the mother who may contract the illness from the viral particles shed through the faeces, Exclusively breastfed babies are at low risk if contracting rotavirus in any case.
I am going to admit that I am passionate about the subject – this is the core of my life
See also Facebook live video
CONCLUSIONS: In a study of women receiving treatment for IBD and their infants, we detected low concentrations of infliximab, adalimumab, certolizumab, natalizumab, and ustekinumab in breast milk samples. We found breastfed infants of mothers on biologics, immunomodulators, or combination therapies to have similar risks of infection and rates of milestone achievement compared with non-breastfed infants or infants unexposed to these drugs. Maternal use of biologic therapy appears compatible with breastfeeding.
With the help of the Breastfeeding and IBD facebook page I wrote this article:
what would you like your healthcare tean to know about IBD and breastfeeding
Finally I have put together all the information on studies on anything to do with prescribing, procedures and vaccines for breastfeeding mums with IBD. If you have IBD take this with you to appointments. If you are a professional please make sure everyone in the team has a copy. I am happy to offer Teams Training to any group of professionals who support mums with IBD.
All you need to know about investigating and treating IBD in breastfeeding mothers factsheet
Live vaccinations and Immunosuppressant medication taken by breastfeeding mothers
To finish the posts on immunosuppresant medications the final most frequently asked question is about the administration of live vaccinations to the baby. This is particularly a problem with the rotavirus vaccine.
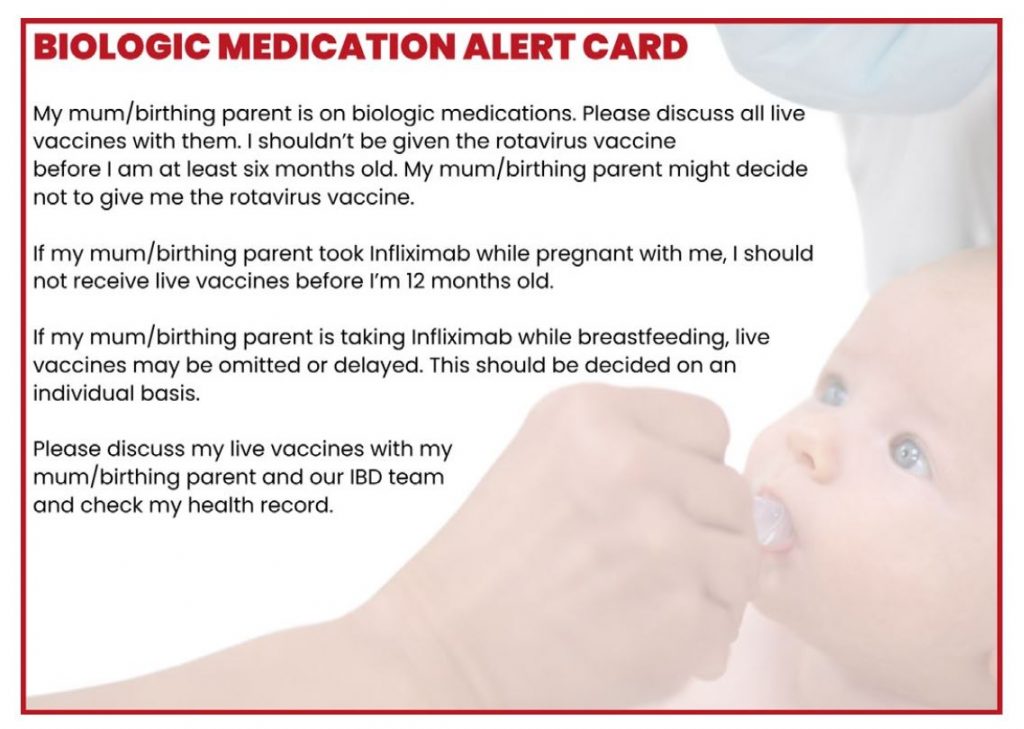
In August 2022 the summary of product characteristics for Infliximab was changed to state that live vaccines should not be administered to the babies of mothers on Infliximab in pregnacy or breastfeeding, before 12 months of age. https://breastfeeding-and-medication.co.uk/wp-content/uploads/2022/10/Infliximab-exposure-in-pregnancy-and-breastfeeding-Aug-2022-update.pdf
The Torento consensus statement recommended that live vaccinations are not recommended within the first 6 months of life in the offspring of women who were on anti-TNF therapy during pregnancy. The babies of mothers taking immunosupressant drugs eg azathioprine and infliximab have not been shown to be immunocompromised because of the limited passage of medication through breastmilk.
However, if live vaccinations, particularly rotavirus are used then the mother with IBD should use precautions like wearing gloves when changing the baby’s nappy for 2 weeks after the vaccination to avoid picking up the particles of live virus shed in faeces.
The Rotavirus Vaccination Programme Public Health England
” There is a potential for transmission of the live attenuated virus in Rotarix vaccine from the infant to severely immunocompromised contacts through faecal material for at least 14 days. However, vaccination of the infant will offer protection to household contacts from wild-type rotavirus disease and outweigh any risk from transmission of vaccine virus to any immunocompromised close contacts. Those in close contact with recently immunised infants should, as always, observe good personal hygiene which should include handwashing after changing the infant’s nappy”
” Rotavirus vaccine should not be given to infants of mothers that used immunosuppressive biological therapy during their pregnancy because of the potential that these will have a postnatal influence on the infants’ immune status. It is recommended that immunisation with live vaccines should be delayed for 6 months in children born to mothers who were on immunosuppressive biological therapy (TNFα antagonists and other biological medicines such as Infliximab) during pregnancy. As Rotarix vaccine is contraindicated in infants presenting for the first dose after 15
weeks of age (beyond 14 weeks and 6 days), infants whose mothers received such treatment during pregnancy will therefore not be eligible to receive Rotarix vaccine, but they should benefit from herd (indirect) protection.”
” Infants born to mothers who received non-biological immunosuppressive therapy such as steroids, cyclosporine, tacrolimus or azathioprine at any time during their pregnancy can safely have the rotavirus vaccine at the appropriate age.
A recent review of the literature concluded that it is safe for mothers to breastfeed while on immune suppression that includes steroids, cyclosporine, tacrolimus or azathioprine. Breastfed infants of mothers taking immunosuppressive therapy can receive rotavirus vaccine at the appropriate age. Rotarix vaccine should not be administered to breastfeeding infants whose mothers are using biological medicines such as Infliximab.”
- Sameh M, Mohsen EK, Jon JK, Halawa A, Sharma Al. Safety of Breastfeeding by Mothers on Immunosuppressive
Medication for Renal Transplantation: Obsession, Myth and Truth. JOJ Uro & Nephron. 2017; 3(3): 555612. Available at
www.juniperpublishers.com/jojun/pdf/JOJUN.MS.ID.555612.pdf
- Public Health England. Immunisation against infectious disease. Contraindications and Special Considerations. Chapter 6.
www.gov.uk/government/publications/contraindications-and-special-considerations-the-green-book-chapter-6
- Nguyen GC, Seow CH, Maxwell C, Huang V, Leung Y, Jones J, Leontiadis GI, Tse F, Mahadevan U, van der Woude CJ The Toronto Consensus Statements for the Management of IBD in Pregnancy. Gastroenterology. 2016;150:734-57
- Julsgaard M, Christensen LA, Gibson PR, Gearry RB, Fallingborg J, Hvas CL, Bibby BM, Uldbjerg N, Connell WR, Rosella O, Grosen A, Brown SJ, Kjeldsen J, Wildt S, Svenningsen L, Sparrow MP, Walsh A, Connor SJ, Radford-Smith G, Lawrance IC, Andrews JM, Ellard K, Bell SJ. Concentrations of Adalimumab and Infliximab in Mothers and Newborns, and Effects on Infection. Gastroenterology. 2016 Jul;151(1):110-9. doi: 10.1053/j.gastro.2016.04.002. Epub 2016 Apr 8. PMID: 27063728.
- Fritzsche J, Pilch A, Mury D, Schaefer C, Weber-Schoendorfer C. Infliximab and adalimumab use during breastfeeding. J Clin Gastroenterol. 2012 Sep;46(8):718-9. doi: 10.1097/MCG.0b013e31825f2807. PMID: 22858514.
Endometriosis and Breastfeeding
Endometriosis is a condition where tissue similar to that lining the womb, starts to grow in other places, such as the ovaries and fallopian tubes. Endometriosis can affect women of any age. The exact number of women who develop endometriosis is unknown. This is because many women have endometriosis without symptoms, or with mild symptoms, and are never diagnosed. Estimates vary, from 1 to 5 in 10 of all women having some degree of endometriosis. Symptoms typically develop between the ages of 25-40 but can begin in teenage years. The condition can run in families.
It can be incredibly painful and hard to live with as evidenced by the mothers in this factsheet who shared their stories. Sadly it is often poorly recognised
Endometriosis and breastfeeding factsheet
My baby is 10 days short of completing 5 months and I got my period last night for the first time post her birth. I had a c-section and at the time of delivery, the gynaecologist found that I have endometriosis level 2 which was the reason for my painful periods before conceiving. This was my first, spontaneous conception and I did not have a clue I have endometriosis.
At my postpartum consultation I was told that as soon as I get my period, I should start my hormonal treatment and also that the hormonal medication is not breastfeeding friendly. I am an EXCLUSIVE BREASTFEEDING mom and want to continue nursing for at least 2 years or until she self-weans. I used to take painkiller, hot water bag and ginger tea for period pain. I came to know I had endometriosis only after I delivered. Biggest thing I have found so far is how symptoms are ignored and women just cope. But I did find that yoga helped me a lot with the symptoms.
I was really worried I would not be able to breastfeed due to the pain medication I took regularly for endometriosis. I was so lucky that the pain I experienced every day for 4 years stopped once I gave birth and was able to go on birth control. The doctor was very informed about what I could and could not take. I’m now a bit scared to stop breastfeeding because I’m worried my periods and pain might return but I will need to stop before going down the frozen embryo route which is a shame as I either stop feeding before I would like or have a larger age gap than I would like.
I have severe dysfunctional uterine bleeding, PCOS and Endometriosis. Possibly adenomyosis. I was put on hormonal treatment 6month post-partum and this resulted in my milk supply depleting within a week, despite the help of domperidone to try to help increase supply. It broke my heart and given the correct information I would have denied medical treatment and continued to breastfeed for as long as possible. But I was misinformed and as a result lost the most precious bond I had. All I can say is I missed out on more than I can put into words. My rainbow boy is healthy and strong, and I am thankful, but I wish I could have done more, changed things, and provided him with the best.
Description
Endometriosis is a condition where tissue similar to that lining the womb, starts to grow in other places, such as the ovaries and fallopian tubes. Endometriosis can affect women of any age. The exact number of women who develop endometriosis is unknown. This is because many women have endometriosis without symptoms, or with mild symptoms, and are never diagnosed. Estimates vary, from 1 to 5 in 10 of all women having some degree of endometriosis. Symptoms typically develop between the ages of 25-40 but can begin in teenage years. The condition can run in families.
The main symptoms of endometriosis are:
- pain in lower tummy or back– usually worse during menstrual period
- period pain that prevents normal activities
- pain during or after sex
- pain when peeing or pooing during menstruation
- feeling sick, constipation, diarrhoea, or blood in your urine during menstruation
- difficulty getting pregnant
Farland et al (2017) studied 72 394 women recruited through the Nurse’s Health Study. The participants had one or more pregnancies that lasted at least six months. Of these women 3296 had laparoscopically confirmed endometriosis. The study found that the duration of total and exclusive breast feeding was significantly associated with decreased risk of endometriosis. For every additional three months of total breast feeding per pregnancy, women experienced an 8% lower risk of endometriosis. Women who breastfed for at least 36 months in total across their reproductive lifetime had a 40% reduced risk of endometriosis compared with women who never breast fed. The authors commented that this association was partially, but not fully, influenced by postpartum amenorrhea
Treatment
There is currently no cure for endometriosis, but symptomatic treatment is available.
Analgesics: paracetamol, opioids (ideally dihydrocodeine or tramadol).
Non-steroidal anti-inflammatory drugs:
- Ibuprofen: very low levels in breastmilk. Can be used even when baby needs direct ibuprofen syrup e.g. during teething or fever
- diclofenac: has historically been widely used in breastfeeding
- naproxen: longer half-life than diclofenac or ibuprofen but levels in breastmilk low
- celecoxib: low levels in breastmilk
the combined pill, the contraceptive patch, or an intrauterine system (IUS/coil) may reduce supply in some.
norethisterone or medroxyprogesterone: may reduce
gonadotrophin-releasing hormone (GnRH) analogues e.g. leuprorelin acetate (Prostrap ™). It is not known whether leuprolide transfers into human milk, but due to its nonapeptide structure, it is not likely that its transfer would be extensive. It is unlikely it would be orally bioavailable in the human infant if ingested via milk. Its effect on lactation is unknown, but it could suppress lactation particularly early postpartum. It is of little risk to the breastfed infant, only to milk production (Hale)
surgery to cut away patches of endometriosis tissue or a hysterectomy
References
Hale TW Medications and Mothers Milk online access
Farland L V, Eliassen A H, Tamimi R M, Spiegelman D, Michels K B, Missmer S A et al. History of breast feeding and risk of incident endometriosis: prospective cohort study BMJ 2017; https://www.bmj.com/content/358/bmj.j3778
Further information
Endometriosis UK: www.endometriosis-uk.org/understanding-endometriosis
Reproduced from Jones W Medication and Chronic Medical Conditions 2020
Indigestion and Gastro-oesophageal reflux disease (GORD) and Breastfeeding
Indigestion (dyspepsia) produces discomfort in the upper stomach, often accompanied by belching and bloating. It is a symptom many of us are familiar with across the Christmas festive period and as a community pharmacist saw most families purchase products in anticipation. Long standing indigestion may be investigated by endoscopy. Symptoms can involve bringing up food or bitter-tasting fluids into your mouth temporarily.
GORD is reflux of the contents of the stomach into the oesophagus. It can also be associated with gastritis (inflammation of the stomach) or damage to the stomach due to use of NSAIDs such as ibuprofen, diclofenac and naproxen. It is associated with the term heartburn and can be linked to a cough. Symptoms can be exacerbated by over-eating, obesity or pregnancy.
H. Pylori can be diagnosed by a test done on a sample of stools (faeces), by a breath test, by a blood test, or from a biopsy sample taken during a gastroscopy (endoscopy). It is treated by a variety of combinations of two antibiotics (clarithromycin, metronidazole and amoxycillin) in high dose plus a PPI for a week. The PPI may be continued for 4-8 weeks.
Treatment
- Antacids containing calcium and sodium – there are many brands available according to choice.
- Simethicone products to absorb wind
- Alginates which form a viscous foam which floats on the stomach contents preventing the reflux
- H2 receptor antagonists such as Famotidine or nizatidine are preferred as smaller amounts pass into breast milk than cimetidine.
- PPIs (proton pump inhibitors) such as omeprazole, lansoprazole, esomeprazole are largely destroyed by stomach acids so little is available to pass into breastmilk
See also SPS Treating heartburn and dyspepsia during breastfeeding
https://www.sps.nhs.uk/articles/treating-heartburn-and-dyspepsia-during-breastfeeding
Irritable Bowel Syndrome (IBS) and breastfeeding
Irritable bowel disease causes distress to many. This factsheet has been developed from my books and particularly Breastfeeding and Chronic Medical Conditions available from Amazon. I hope it helps.
wendy@breastfeeding-and-medication.co.uk
In October 2023 a new paper (https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(23)01725-7/fulltext) was published on the use of low dose amitriptyline to treat IBS if anti smasmodic agents have failed to control symptoms. Amitriptyline is compatible with breastfeeding but care should be taken co-sleeping as it may cause maternal drowsiness.
“
IBS is increasingly managed in primary care, commonly with analgesics and dietary regimes as first-line approaches. Although psychotropic drugs such as tricyclic antidepressants and selective serotonin reuptake inhibitors have shown effectiveness as second-line treatment for IBS, their use is not widespread in primary practice. Tricyclic antidepressants, such as amitriptyline or desipramine, are advocated at low doses to relieve IBS symptoms, but so far there is no solid evidence for their effectiveness and safety in primary care.
Alexander C Ford and colleagues conducted the ATLANTIS randomised controlled trial in adult patients with IBS in primary care in the UK, comparing amitriptyline at doses of 10 mg to 30 mg once daily with placebo. Patients were required to meet Rome IV diagnostic criteria, and have ongoing symptoms with an IBS Severity Scoring System (IBS-SSS) score of greater than or equal to 75 despite dietary changes and first-line treatments. Patients, general practitioners, and the research team were masked for the trial medication, which is essential in IBS research, given the high placebo response in the condition. Symptom-based, subjective, and social outcome measures, including anxiety and depression, were used, in line with the broad disease effect of IBS. The primary endpoint was the IBS-SSS score at 6 months. Outcomes were measured at months 3, 6, and 12, but the month 12 outcomes had a lower sample size than intended owing to follow-up being curtailed by the COVID-19 pandemic.
The results of the ATLANTIS trial are robust and consistent, and demonstrate that a low dose tricyclic antidepressant can be effectively and safely applied for patients with IBS in primary care, as an option, not as standard treatment. Optimal IBS management requires a personalised approach, with treatment steps dependent on the type of IBS symptoms, disease history, treatment response in the past, and sensitivity to side-effects.
Irritable bowel syndrome can be treated during breastfeeding. Some remedies suit some mothers more than other remedies. There is also a significant body of research that indicates that CBT is effective in reducing IBS symptoms of abdominal pain, diarrhoea, and constipation.
See also SPS Using gastrointestinal antispasmodics during breastfeeding https://www.sps.nhs.uk/articles/using-gastrointestinal-antispasmodics-during-breastfeeding/
Introduction
Irritable bowel syndrome (IBS) is a common, chronic, relapsing, and often life-long condition, mainly affecting people aged between 20 and 30 years. It is more common in women. Symptoms include abdominal pain or discomfort, either diarrhoea or constipation (or both alternating) and bloating. The treatment of IBS is focused on symptom control, in order to improve quality of life. It occurs in 10-20% of the population and again is more common in women than men.
Diagnosis
According to NICE CG 61 (Irritable bowel syndrome in adults: diagnosis and management) in order to diagnose IBS:
Patients must give at least a six-month history of either:
• Abdominal pain or discomfort.
• Bloating.
• Change in bowel habit. Consider positively diagnosing IBS only if abdominal pain is either relieved by defecation or associated with altered bowel frequency or stool form.
AND at least 2 of the following are present:
Altered passage of stool (straining, urgency, incomplete evacuation).
• Abdominal bloating (women >men), distention tension or hardness.
• Symptoms aggravated by eating.
• Passage of mucus rectally.
Before diagnosis, blood tests and a colonoscopy are commonly undertaken to rule out other conditions which may, at least initially, present with similar symptoms e.g., IBD.
Medication
The categories of drugs involved reduce spasms, control constipation or diarrhoea (see section on bowel issues). Symptoms are frequently accompanied by depression.
Dicycloverine (Dicyclomine) (Merbentyl ™ Kolanticon ™). In the past this drug was used to treat colic in babies but following reports of breathing difficulties, its license for use in infants under 6 months was withdrawn. The adverse reactions occurred in babies under the age of 6 weeks and involved sudden reactions following administration of the drug via a spoon. All children recovered normally (Williams 1994, Edwards 1984, Spoudea 1984). There is also a single case report of a similar reaction in a 12-day old, breastfed baby whose mother took this drug (personal communication reported in Briggs 2005), so it is a drug best avoided in lactation since there are alternative preparations available.
Hyoscine (Buscopan ™) is often the drug preferred by patients with IBS. No levels in breastmilk have been reported from studies. It is licensed at half the adult dose for children over 6 years (10 milligrams three times daily) so the amount passing into breastmilk is likely to be safe.
Alverine (Relaxyl™, Spasmonal™) is widely used to treat symptoms of irritable bowel syndrome but one study shows that it was no better than placebo in providing relief of symptoms (Mitchell 2002). It is licensed for use in patients over the age of 12 years. There is no information on its passage into breastmilk. Avoid if possible.
Mebeverine (Colofac™) should be taken 20 minutes before meals for maximum effect. It is licensed for use in children above the age of three so levels passing into breastmilk are likely to be safe.
Peppermint Oil (Colpermin ™) capsules are used to relieve spasms associated with IBS but should be swallowed whole, half to one hour before food to avoid irritation of the oesophagus. There is some evidence to support the value of this product in therapy (Pittler 1998, Grigoleit 2005). Peppermint oil is believed to undergo rapid first pass metabolism so levels in breastmilk will be low. There have been anecdotal reports in internet discussions by lactation specialists in the US that it can reduce milk supply but there are currently no studies to prove or disprove these.
References
• De Wit N Low-dose amitriptyline in irritable bowel syndrome: ready for primary care? The Lancet Oct 2023.
- Edwards PDL. Dicyclomine in babies. BMJ 1984; 288: 1230. Reported as personal communication in Briggs GG, Freeman RK, and Yaffe SJ. Drugs in pregnancy and lactation, 7th ed. Baltimore. Williams & Wilkins. 2005
• Grigoleit H-G, Grigoleit P. Peppermint oil in irritable bowel syndrome. Phytomedicine 2005; 12: 601-6
• Hale T W Medications and Mothers Milk
• Jones W Breastfeeding and Medication (Routledge 2018)
• LactMed database http://toxnet.nlm.nih.gov/cgi-bin/sis/htmlgen?LACTMED
• Mitchell SA, Mee AS, Smith GD, Palmer KR, Chapman RW. Alverine citrate fails to relieve the symptoms of irritable bowel syndrome: results of a double-blind, randomized, placebo-controlled trial. Aliment Pharmacol Ther. 2002 16(6):1187-95.
• NICE QS 114 (2016) Irritable bowel syndrome in adults
• Pittler MH, Ernst E. Peppermint oil for irritable bowel syndrome: a critical review and meta-analysis. Am J Gastroenterol 1998; 93: 1131-5.
• Spoudeas H, Shribman S. Dicyclomine in babies. BMJ 1984; 288: 1230
• Williams J, Watkin-Jones R. Dicyclomine: worrying symptoms associated with its use in some small babies. BMJ 1984; 288: 90
Further information
The IBS Network https://www.theibsnetwork.org/
Sleep problems when breastfeeding
One of the hardest questions I have to answer. I want to help but I need to keep the breastfed baby safe too
See also SPS Treating insomnia during breastfeeding
www.sps.nhs.uk/articles/treating-insomnia-during-breastfeeding
Sleeping tablets and breastfeeding factsheet
Being asked about the safety of sleeping tablets by a breastfeeding mum is probably one of the hardest questions there is. My first problem is that I was taught as a pharmacist that sleeping tablets should only be used very short term and as a last resort. They are highly addictive. They do not solve problems long term. My second problem is that in order to induce sleep they have to cross the blood brain barrier and can therefore cause drowsiness in the baby from the amount passing through milk. The third problem is who will be looking after the baby during the night – will it be fed by someone else? Does the mum co sleep in which case how can we keep the baby safe? If mum is going to get up to feed the baby is there a risk that she will fall asleep on the sofa which is an even greater risk of SIDS.
Most mothers who ask about the use of sleeping tablets are suffering from anxiety or depression. It is a chicken and egg situation – does the lack of sleep cause anxiety/depression or is the inability to sleep a symptom of the anxiety/depression?
Many people find that they can be helped to sleep by using the self-hypnosis sites similar to those used for labour and hypno-birthing. Others by meditation or mindfulness and I cannot praise the Headspace app enough. These practices may take several days to work and are not an instant cure for lack of ability to sleep but they do not affect breastfeeding.
Some people find that herbs such as Valerian help. There is limited research on safety but anecdotally they do not appear to cause drowsiness in the baby. LactMed states that “ Valerian has no specific uses in nursing mothers, but is most commonly used to treat anxiety and sleep disturbances, and occasionally for self-treatment of postpartum blues or depression. No data exist on the safety and efficacy of valerian in nursing mothers or infants. In general, valerian is well tolerated, with side effects such as dizziness, hangover or headache reported occasionally. Valerian is “generally recognized as safe” (GRAS) for use in food by the U.S. Food and Drug Administration. Valerian is often not recommended during lactation because of the theoretical concerns over its valepotriates and baldrinals which have been shown to be cytotoxic and mutagenic in vitro. Because there is no published experience with valerian during breastfeeding, an alternate therapy may be preferred, especially while nursing a newborn or preterm infant.”
Symptoms of anxiety is better managed by the use of SSRI antidepressants and/or betablockers such as propranolol both of which pass into milk in very low levels. The gold standard is CBT therapy
https://www.breastfeedingnetwork.org.uk/factsheet/anxiety/
Depression can be managed by the use of SSRI antidepressants and CBT
https://breastfeeding-and-medication.co.uk/fact-sheet/depression-and-breastfeeding-2
Prescribed sleeping tablets
Insomnia is defined as the inability to achieve or maintain sleep. It may occur short term or become chronic. Insomnia may be a manifestation of an underlying condition such as depression or anxiety. The use of hypnotics is generally only recommended at the lowest effective dose for as short a period as possible with an emphasis on sleep hygiene and non-pharmacological measures. Tolerance develops within a very short space of time (3–14 days). Benzodiazepines are generally regarded as the drugs of first choice. Dependence can become a problem with regular or frequent use and withdrawal leads to rebound insomnia. Use during lactation should be discouraged, as the mother may be unresponsive to the needs of the baby. Co-sleeping after taking sedatives produces an increased risk of SIDS (see Caring for your baby at night, Baby Friendly UK 2017, www.unicef.org.uk/BabyFriendly/Resources-for-parents/Caring-for-your-baby-at-night).
Zopiclone : has similar sedative and anxiolytic activity to those of the benzodiazepines. It is claimed to initiate sleep rapidly, without reduction of total rapid-eye-movement (REM) sleep. Matheson et al. (1990) studied 12 women who took a single dose of zopiclone 7.5 mg in the early post-natal period. They found low levels of transfer via breastmilk equivalent to 1.4% of the weight-adjusted maternal dose. The babies were not allowed to breastfeed for up to ten hours but displayed no adverse effects when they resumed breastfeeding. The BNF reports that it is secreted into breastmilk and that it should be avoided.
Reference
- Matheson I, Sande HA, Gaillot J, The excretion of zopiclone into breastmilk, Br J Clin Pharmacol, 1990;30:267–71.
Zolpidem: an imidazopyridine with similar sedative properties to the benzodiazepines but minimal anxiolytic properties. It has a rapid onset and a short duration of action, and is used as a hypnotic in the short-term management of insomnia. It undergoes first-pass metabolism and has an oral bio-availability of 70%. It is 92% bound to plasma proteins. Hale reports a personal communication case report of a baby who became excessively somnolent when its mother took 100 mg sertraline and 10 mg zolpidem, which resolved when the hypnotic was discontinued (Hale 2017 online access). In five women given a 20-mg dose of zolpidem (normal dose 10 mg), after three hours the amount of drug detected in breastmilk ranged between 0.76 and 3.88 µg. This is taken to indicate the peak level to which the baby would be exposed (Pons et al. 1989). No detectable zolpidem was found in subsequent milk samples. The BNF reports that there is only a small amount secreted into breastmilk but that it should be avoided.
References
- Reported in Hale T, Medications and Mothers’ Milk (2010) as a personal communication.
- Pons G, Francoual C, Guillet P, Moran C, Hermann P, Bianchetti G, Thiercelin JF, Thenot JP, Olive G, Zolpidem excretion in breastmilk, Eur J Clin Pharmacol, 1989;37:245–8.
Temazepam: is 96% plasma protein bound. It is a short-acting benzodiazepine with a half-life reportedly between 8 and 15 hours. It is used in short-term management of insomnia but should not be used for more than 14–28 days. Lebedevs et al. (1992) studied ten women all with babies less than 15 days old. The mothers were given 10–20 mg for two nights before milk levels were studied. No adverse effects were noted in any of the babies. Temazepam levels were detected in breastmilk in only one of the ten mothers. The authors considered that breastfed neonates would ingest negligible amounts of temazepam. It is not licenced for use in children. The BNF recommends that benzodiazepines are present in milk, and should be avoided if possible during breastfeeding.
Reference
- Lebedevs TH, Wojnar-Horton RE, Yapp P, Roberts MJ, Dusci LJ, Hackett LP, Ilett KF, Excretion of temazepam in breastmilk, Br J Clin Pharmacol, 1992;33:204–6.
Nitrazepam: Matheson et al. (1990) studied nine women who received 5 mg nitrazepam nightly for five nights. No adverse effects were noted in the infants. The average amount of nitrazepam received by the breastfed baby in the morning was calculated to increase from 1 to 1.5 µg per 100 millilitres. The authors concluded that nitrazepam was compatible with breastfeeding in the immediate post-natal period but that further studies were necessary to confirm safety in the longer term. Relative infant dose is quoted as 2.9% (Hale 2017 online access). It is not licenced for use in children. It is 87% plasma protein bound. Half-lives of 24–30 hours have been reported (Martindale 2017). The BNF recommends that benzodiazepines are present in milk and should be avoided if possible during breastfeeding.
Reference
- Matheson I, Lunde PK, Bredesen JE, Midazolam and nitrazepam in the maternity ward: milk concentrations and clinical effects, Br J Clin Pharmacol, 1990;30:787–93.
Prescribed sedatives for anxiety
Diazepam: Diazepam has a long half-life (with terminal metabolite being present for two to five days) and accumulation is possible. The plasma elimination is further extended in neonates due to poor hepatic function. It is 98% plasma protein bound. A shorter-acting anxiolytic is preferable for use for more than a few days, particularly in neonates. Brandt (1976) conducted a study of four post-natal women who were given 10 mg diazepam at bedtime for six nights. He concluded that even with a neonate, a maternal dose of 10 mg produced breastmilk levels too small to cause any untoward effects in the baby. Erkkola and Kanto (1972) studied three infants whose mothers were taking 10 mg diazepam three times daily from delivery. The babies were observed for six days during which period no symptoms of sedation were noticed. However, Patrick et al. (1972) reported on a single mother taking the same dose. At 8 days of age (three days after the mother commenced diazepam) symptoms of lethargy, EEG changes and weight loss were apparent in the infant and attributed to the diazepam exposure. Relative infant dose quoted as 7.1% (Hale 2017 online access). It is licenced for use in children only to control convulsions. Diazepam is also a drug that may be abused in large doses. Close observation of the baby should be undertaken and the mother encouraged to reduce the dosage as far as possible under supervision of a detoxification service if necessary. The BNF suggests that benzodiazepines are present in milk and should be avoided if possible during breastfeeding. Diazepam is used to relieve muscular spasm following back injuries and use for a short period of time should not preclude it from use by lactating mothers in these circumstances. However, babies should be observed for sedation. Single doses of diazepam may also be used in situations such as fear of flying, before surgery or other anxiety-provoking situations with continued breastfeeding as normal
References
- Brandt R, Passage of diazepam and desmethyldiazepam into breastmilk, Arzneimittelforschung, 1976;26:454–7.
- Erkkola R, Kanto J, Diazepam and breastfeeding, The Lancet, 1972;299:1235–6, Letter.
- Patrick MJ, Tilstone WJ, Reavey P, Diazepam and breastfeeding, The Lancet, 1972;299:542–3, Letter.
Alprazolam (Xanax): a benzodiazepine but is preferred due to the shorter half-life (12–15 hours). Oo et al. (1995) obtained multiple milk and serum samples from eight lactating subjects up to 36 hours after a single oral dose of 0.5 mg alprazolam. The milk plasma ratio was determined to be 0.36, a level too low to produce clinically significant levels. No outcomes were available as the infants were not breastfed. Reports of withdrawal in infants exposed in utero and breastfed are documented (Anderson and McGuire 1989). Hale quotes a relative infant dose of 8.5% (Hale 2017 online access). The BNF states that all benzodiazepines are present in milk and should be avoided if possible during breastfeeding.
References
- Oo CY, Kuhn RJ, Desai N, Wright CE, McNamara PJ, Pharmacokinetics in lactating women: prediction of alprazolam transfer into milk, Br J Clin Pharmacol, 1995;40(3):231–6.
- Anderson PO, McGuire GG, Neonatal alprazolam withdrawal—possible effects of breast feeding, DICP, 1989;23(7–8):614.
Lorazepam: is 85% bound to plasma proteins and is 90% bio-available. Half-life is reported as 10 to 20 hours. A post-partum study (Summerfield and Nielsen 1985) found clinically insignificant amounts of lorazepam in breastmilk even at a dose of 2.5 mg twice daily for the first five days post-natally. Whitelaw et al. (1981) estimated that an exclusively breastfed infant would be exposed to 7 µg per kilogramme per day with a maternal dose of 2.5 mg twice daily The single infant studied showed no signs of sedation. The dose used in this study is more than the usual maximum of 2 mg daily. Relative infant dose is quoted as 2.5% (Hale 2017 online access). It is licenced for use in children only to control convulsions. The BNF suggests that benzodiazepines are present in milk and should be avoided if possible during breastfeeding. LactMed reports that lorazepam has low levels in breastmilk, a short half-life relative to many other benzodiazepines, and is safely administered directly to infants. Evidence from nursing mothers indicates that lorazepam does not cause any adverse effects in breastfed infants with usual maternal dosages and that no special precautions are required. Using Kelly (2012) data lorazepam may be taken as one of the safest benzodiazepines if use is important.
References
- Kelly LE, Poon S, Madadi P, Koren G, Neonatal benzodiazepines exposure during breastfeeding, J Pediatr, 2012;161:448–51.
- Summerfield RJ, Nielsen MS, Excretion of lorazepam into breastmilk, Br J Anaesth, 1985; 57:1042–3.
- Whitelaw AG, Cummings AJ, McFadyen IR, Effect of maternal lorazepam on the neonate, BMJ (Clin Res Ed), 1981;282(6270):1106–8.
MMR Vaccine and Breastfeeding
As the MMR cases continue to spread I am aware that adults without documented vaccine are being called in to receive their immunisation especially in areas where cases are high like Birmingham and London.
If you are breastfeeding you can have the MMR jab and breastfeed as normal.
From the Green Book https://assets.publishing.service.gov.uk/media/5e021b9140f0b6665e80187b/Greenbook_chapter_21_Measles_December_2019.pdf
“Breast-feeding is not a contraindication to MMR. Immunisation, and MMR vaccine can be given to breast-feeding mothers without any risk to their baby. Very occasionally, rubella vaccine virus has been found in breast milk, but this has not caused any symptoms in the baby (Buimovici-Klein et al., 1997; Landes et al., 1980; Losonsky et al., 1982). The vaccine does not work when taken orally. There is no evidence of mumps and measles vaccine viruses being found in breast milk.”
MMR vaccine is not recommended for patients with severe immunosuppression as it is a live vaccine
Ankylosing spondylitis and Breastfeeding
From my book Breastfeeding and Chronic Medical Conditions available on Amazon
“From a slightly alternative angle… I have ankylosing spondylitis, thankfully mild. I used to have quite bad pain and stiffness in the mornings and was fairly reliant on NSAIDs. Since breastfeeding (6 years continuously over 2 children now!) these symptoms are basically gone! I put it down to being pretty “active” feeding overnight so do not get a chance to stiffen up!“
“I have a chronic degenerative back condition called ankylosing spondylitis. Breastfeeding was difficult once my condition returned 3 months after birth (was in remission in pregnancy) especially when he was cluster feeding, sitting and not moving for long periods of time caused intense pain but I did what I had to give my boy the best I could. I have also had to try different medications as breastfeeding meant I could not take what I was taking before being pregnant. My little boy is now 8 months old and I could not be more proud that I am still breastfeeding“
Description
Ankylosing spondylitis is a chronic arthritic condition in which the spine and other areas of the body become inflamed. It commonly develops in teenagers and young adults. It is twice as common in men as in women. Back pain and stiffness last at least 30 minutes and then eases through the day or with activity. Commonly the pain causes night waking. Some sources describe pain in one or both buttocks and sometimes the backs of the thighs.
Symptoms include pain and swelling in other parts of the body: inflammation of the joints and where a tendon joins a bone as well as extreme fatigue.
Treatment
- Exercise and physiotherapy to improve movement.
- NSAIDs – ibuprofen, diclofenac, and naproxen all of which are compatible with breastfeeding.
- Anti TNF medication – adalimumab, Certolizumab pegol, Etanercept, Golimumab and Infliximab. These are large molecules which cannot be absorbed from breastmilk.
- Steroid tablets and injections into affected joints which are compatible with breastfeeding
- Assessment of risk of osteoporosis and treatment where necessary. See Section on Osteoporosis.
Further Information:
National Axial Spondylarthritis Society https://nass.co.uk/